Wellcare Inpatient Authorization Form
Wellcare Inpatient Authorization Form - If you want to fill out this form pdf, our document editor is what you need! Select authorization appeal from the drop down. Web to appeal an authorization in denied status, search for the authorization using one of these criteria: Web children and family treatment supports services continuing authorization request form if the mco is requesting concurrent review before the fourth visit; Web enter your official identification and contact details. >>complete your attestation today!<< disputes, reconsiderations and grievances appointment of representative. Web wellcare prior prescription (rx) authorization form. Authorizations are valid for the. Authorization determinations are made based on medical necessity and appropriateness and reflect the application of wellcare’s review criteria guidelines. Web inpatient authorization request in order to ensure our members receive quality care, appropriate claims payment, and notification of servicing providers, please complete this form in its entirety.
Web enter your official identification and contact details. Web this form is intended solely for pcp requesting termination of a member (refer to wellcare provider manual). Authorization requirements are available in the quick reference guide (qrg). Search results will display based on date of service. Web children and family treatment supports services continuing authorization request form if the mco is requesting concurrent review before the fourth visit; Prior authorization request form (pdf) inpatient fax cover letter (pdf) Please type or print in black ink and submit this request to the fax number below. Determination made as expeditiously as the enrollee’s health condition requires, but no later than 14 calendar days after the receipt of request. Web inpatient authorization request in order to ensure our members receive quality care, appropriate claims payment, and notification of servicing providers, please complete this form in its entirety. Web forms | wellcare forms providers medicare overview forms forms access key forms for authorizations, claims, pharmacy and more.
Authorization requirements are available in the quick reference guide (qrg). Web to appeal an authorization in denied status, search for the authorization using one of these criteria: The cftss provider can complete this form when requesting continuation of services. The wellcare prescription drug coverage determination form can be used for prior authorization requests, the demand by a healthcare practitioner that their patient receive coverage for a medication that they deem necessary to their recovery. Web the wellcare prior authorization form is a way for patients to get physician approval prior to receiving services. >>complete your attestation today!<< disputes, reconsiderations and grievances appointment of representative. Select authorization appeal from the drop down. Apply a check mark to point the choice where demanded. Search results will display based on date of service. Member/subscriber id, provider id, patient name and date of birth, medicare id or medicaid id.
Free Wellcare Prior Prescription (Rx) Authorization Form PDF
Authorization determinations are made based on medical necessity and appropriateness and reflect the application of wellcare’s review criteria guidelines. The wellcare prescription drug coverage determination form can be used for prior authorization requests, the demand by a healthcare practitioner that their patient receive coverage for a medication that they deem necessary to their recovery. Web wellcare prior prescription (rx) authorization.
Fillable Outpatient Notification /authorization Request Wellcare
Search results will display based on date of service. February 13, 2023 by tamble. Web children and family treatment supports services continuing authorization request form if the mco is requesting concurrent review before the fourth visit; Member/subscriber id, provider id, patient name and date of birth, medicare id or medicaid id. If you want to fill out this form pdf,.

Central Health Medicare Plan Otc Order Form Form Resume Examples
By clicking on the button down below, you will access the page where you'll be able to edit, save, and print your document. Web this form is intended solely for pcp requesting termination of a member (refer to wellcare provider manual). Authorization requirements are available in the quick reference guide (qrg). >>complete your attestation today!<< disputes, reconsiderations and grievances appointment.
Wellcare Forms For Prior Authorization Fill Out and Sign Printable
Complete this request in its entirety and attach all supporting documentation, including pertinent medical records and office notes Web inpatient authorization request in order to ensure our members receive quality care, appropriate claims payment, and notification of servicing providers, please complete this form in its entirety. Web wellcare prior prescription (rx) authorization form. By clicking on the button down below,.
Fillable Tricare For Life Authorization Request Form Skilled Nursing
Web if you provide services such as primary care, specialist care, mental health, substance abuse and more, please download and complete the forms below: Select authorization appeal from the drop down. Complete this request in its entirety and attach all supporting documentation, including pertinent medical records and office notes >>complete your attestation today!<< access key forms for authorizations, claims, pharmacy.
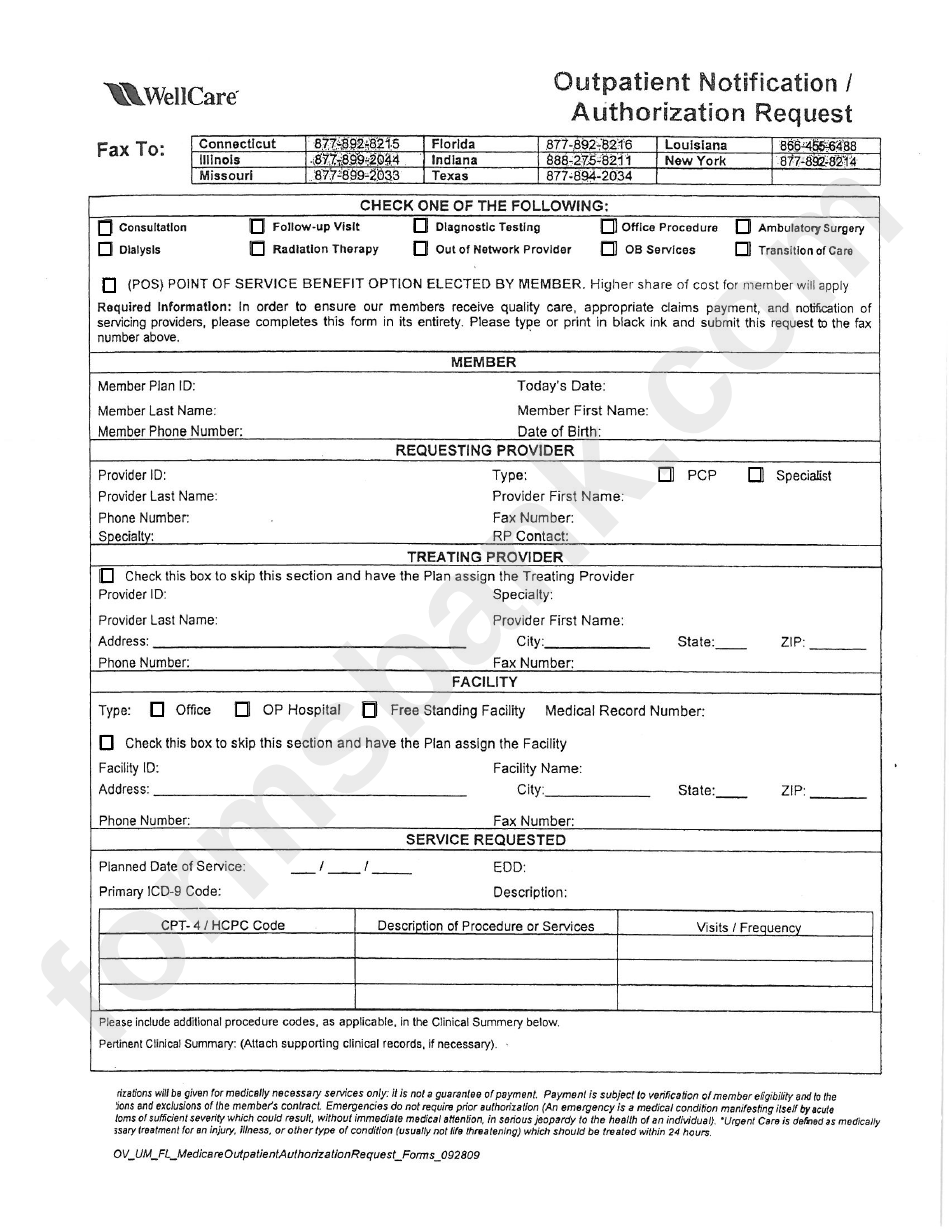
Fillable Outpatient Notification /authorization Request Wellcare
February 13, 2023 by tamble. Web wellcare outpatient authorization request form. Select authorization appeal from the drop down. Double check all the fillable fields to ensure complete accuracy. >>complete your attestation today!<< disputes, reconsiderations and grievances appointment of representative.
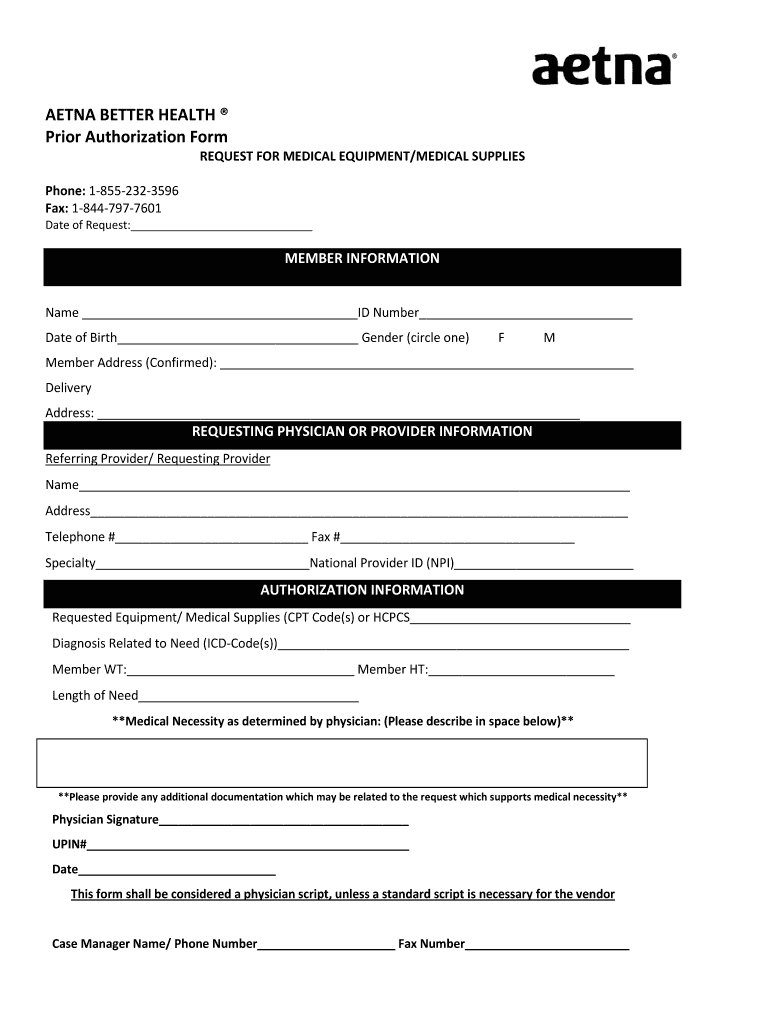
Aetna Better Health Prior Authorization Fill and Sign Printable
Member/subscriber id, provider id, patient name and date of birth, medicare id or medicaid id. Web children and family treatment supports services continuing authorization request form if the mco is requesting concurrent review before the fourth visit; Prior authorization request form (pdf) inpatient fax cover letter (pdf) Apply a check mark to point the choice where demanded. The wellcare prescription.

Wellcare Medicare Part D Medication Prior Authorization Form Form
Utilize the sign tool to add and create your electronic signature to signnow the well care prior authorization form medicare part d. Authorizations are valid for the. Web authorizations | wellcare providers medicare overview authorizations authorizations providers must obtain prior authorization for certain services and procedures. Double check all the fillable fields to ensure complete accuracy. Member/subscriber id, provider id,.
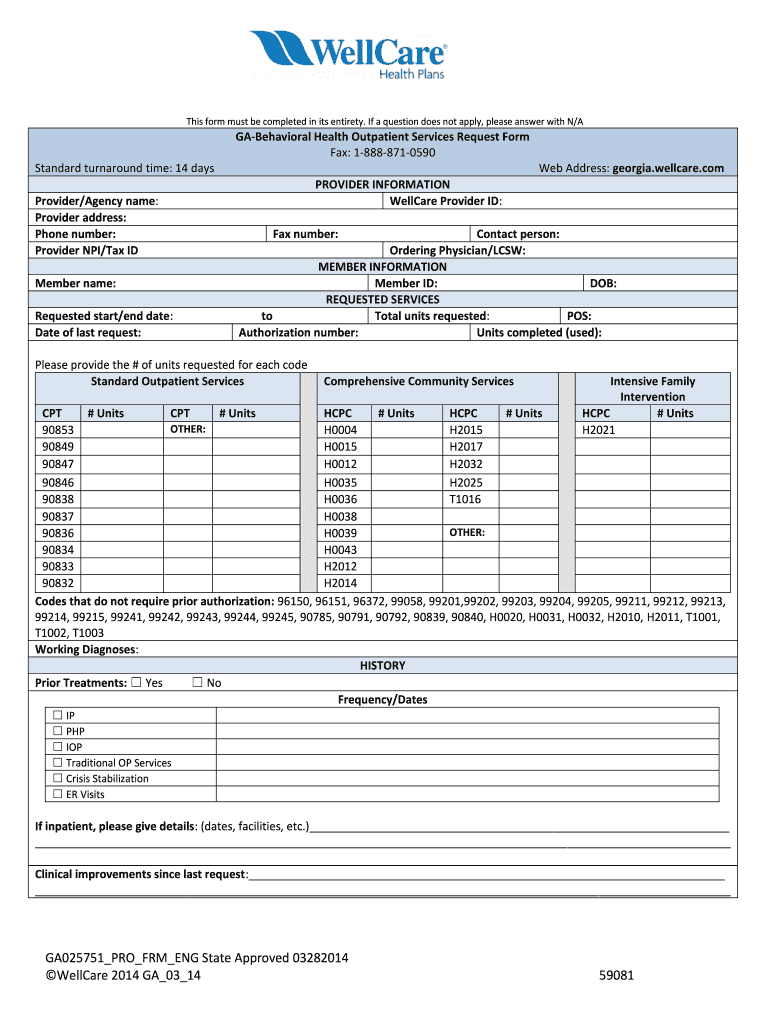
Wellcare Behavioral Health Service Request Form Fill Out and Sign
Determination made as expeditiously as the enrollee’s health condition requires, but no later than 14 calendar days after the receipt of request. Authorization requirements are available in the quick reference guide (qrg). Web wellcare prior prescription (rx) authorization form. Web authorizations | wellcare providers medicare overview authorizations authorizations providers must obtain prior authorization for certain services and procedures. Utilize the.
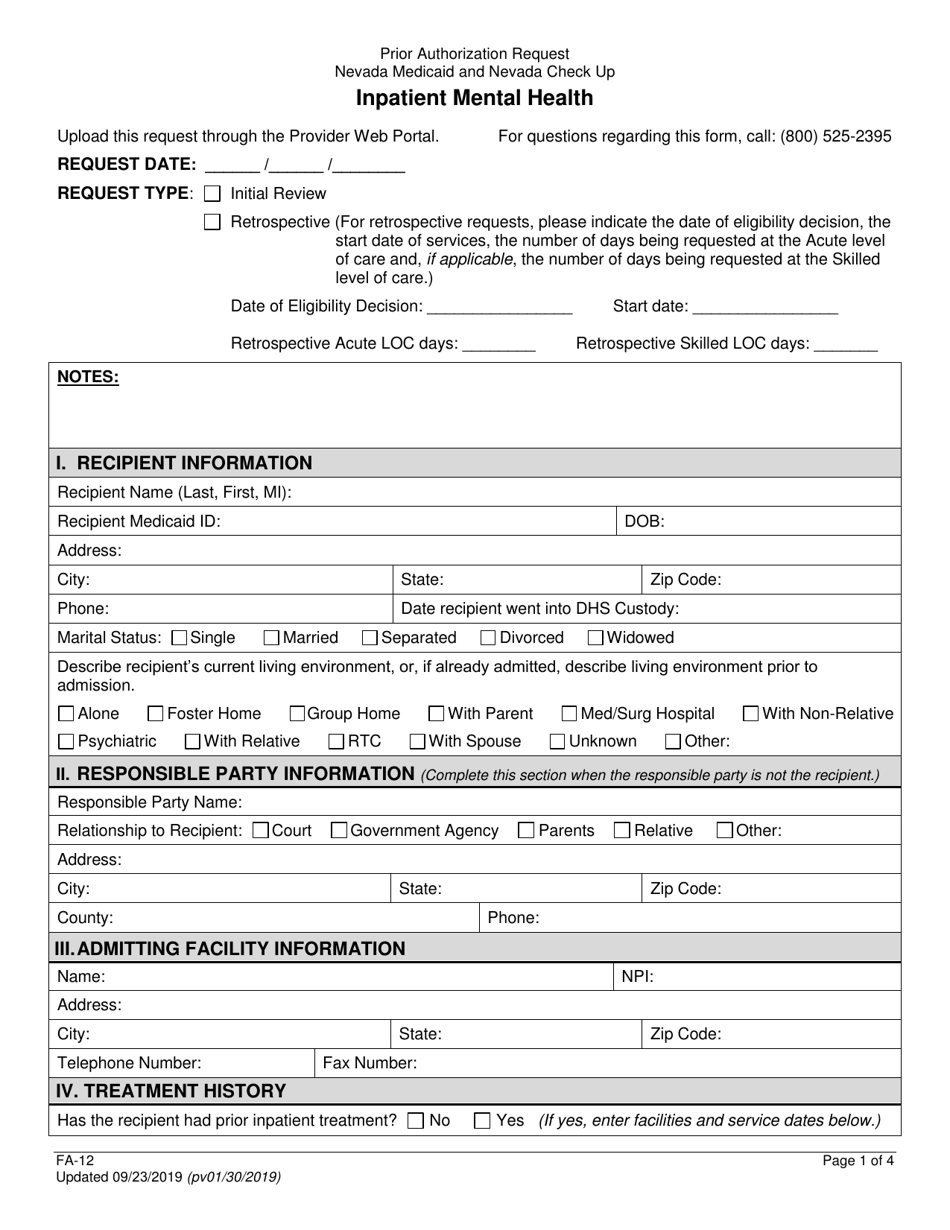
Form FA12 Download Fillable PDF or Fill Online Inpatient Mental Health
Authorization determinations are made based on medical necessity and appropriateness and reflect the application of wellcare’s review criteria guidelines. Apply a check mark to point the choice where demanded. Prior authorization request form (pdf) inpatient fax cover letter (pdf) Please type or print in black ink and submit this request to the fax number below. The wellcare prescription drug coverage.
Web Inpatient Authorization Request In Order To Ensure Our Members Receive Quality Care, Appropriate Claims Payment, And Notification Of Servicing Providers, Please Complete This Form In Its Entirety.
Web wellcare outpatient authorization request form. Member/subscriber id, provider id, patient name and date of birth, medicare id or medicaid id. Please type or print in black ink and submit this request to the fax number below. Web this form is intended solely for pcp requesting termination of a member (refer to wellcare provider manual).
The Wellcare Prescription Drug Coverage Determination Form Can Be Used For Prior Authorization Requests, The Demand By A Healthcare Practitioner That Their Patient Receive Coverage For A Medication That They Deem Necessary To Their Recovery.
>>complete your attestation today!<< disputes, reconsiderations and grievances appointment of representative. Select authorization appeal from the drop down. Web wellcare prior prescription (rx) authorization form. Web to appeal an authorization in denied status, search for the authorization using one of these criteria:
Authorizations Are Valid For The.
Utilize the sign tool to add and create your electronic signature to signnow the well care prior authorization form medicare part d. Web authorization form standard requests: Double check all the fillable fields to ensure complete accuracy. Search results will display based on date of service.
If You Want To Fill Out This Form Pdf, Our Document Editor Is What You Need!
Determination made as expeditiously as the enrollee’s health condition requires, but no later than 14 calendar days after the receipt of request. >>complete your attestation today!<< access key forms for authorizations, claims, pharmacy and more. Web if you provide services such as primary care, specialist care, mental health, substance abuse and more, please download and complete the forms below: Authorization requirements are available in the quick reference guide (qrg).