Wellcare Appeal Form
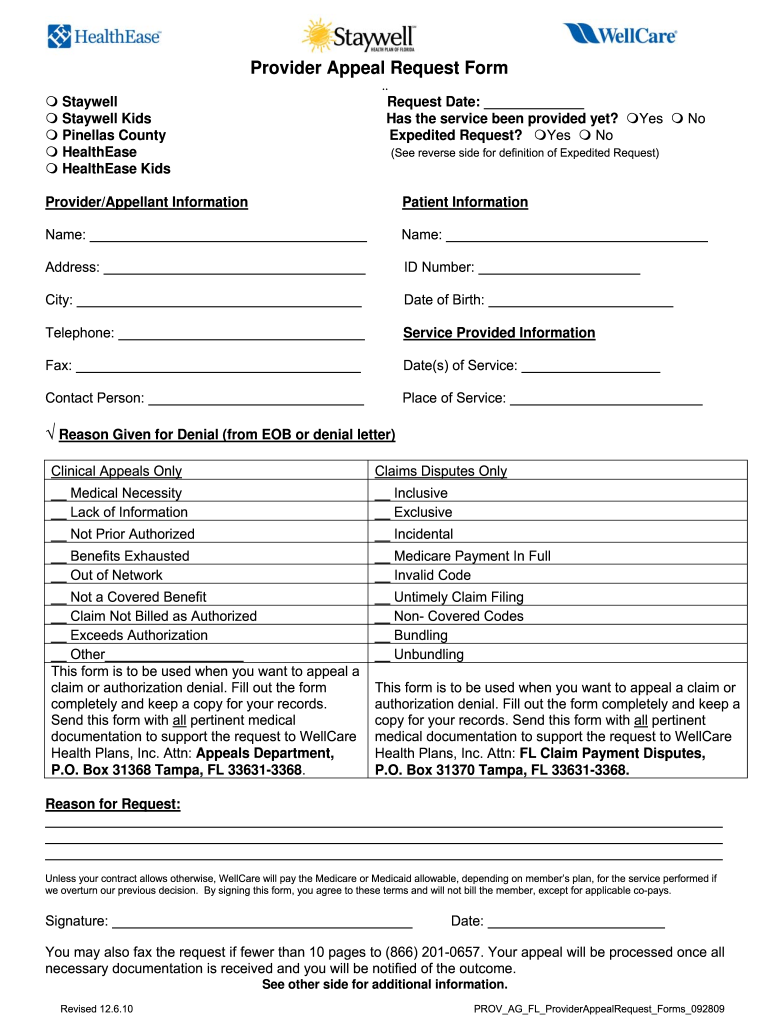
Wellcare Appeal Form - How long do i have to submit an appeal? What is the procedure for filing an appeal? Do not attach original claim form.) Web medication appeal request form you can use this form to request an appeal when a medication coverage determination request has been denied. Please do not include this form with a corrected claim. An expedited redetermination (part d appeal) request can be made by phone at contact us or refer to the number on the back of your member id. To access the form, please pick your state: Contact us, or refer to the number on the back of your wellcare member id card. (attach medical records for code audits, code edits or authorization denials. Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc.
Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. You can now quickly request an appeal for your drug coverage through the request for redetermination form. Access key forms for authorizations, claims, pharmacy and more. Please do not include this form with a corrected claim. Contact us, or refer to the number on the back of your wellcare member id card. Prior authorization request form (pdf) inpatient fax cover letter (pdf) medication appeal request form (pdf) medicaid drug coverage request form (pdf) notice of pregnancy form (pdf) provider incident report form (pdf) pcp change request form for prepaid health plans (phps) (pdf) How long do i have to submit an appeal? (attach medical records for code audits, code edits or authorization denials. Missouri care health plan attn: Complete an appeal of coverage determination request (pdf) and send it to:
Do not attach original claim form.) Appeals 4205 philips farm road, suite 100 columbia, mo 65201. (attach medical records for code audits, code edits or authorization denials. Contact us, or refer to the number on the back of your wellcare member id card. Web request for redetermination of medicare prescription drug denial (appeal) (pdf) this form may be sent to us by mail or fax: How long do i have to submit an appeal? Prior authorization request form (pdf) inpatient fax cover letter (pdf) medication appeal request form (pdf) medicaid drug coverage request form (pdf) notice of pregnancy form (pdf) provider incident report form (pdf) pcp change request form for prepaid health plans (phps) (pdf) Web claim” process in the wellcare by allwell provider manual, found on superiorhealthplan.com/providermanuals. Access key forms for authorizations, claims, pharmacy and more. We have redesigned our website.
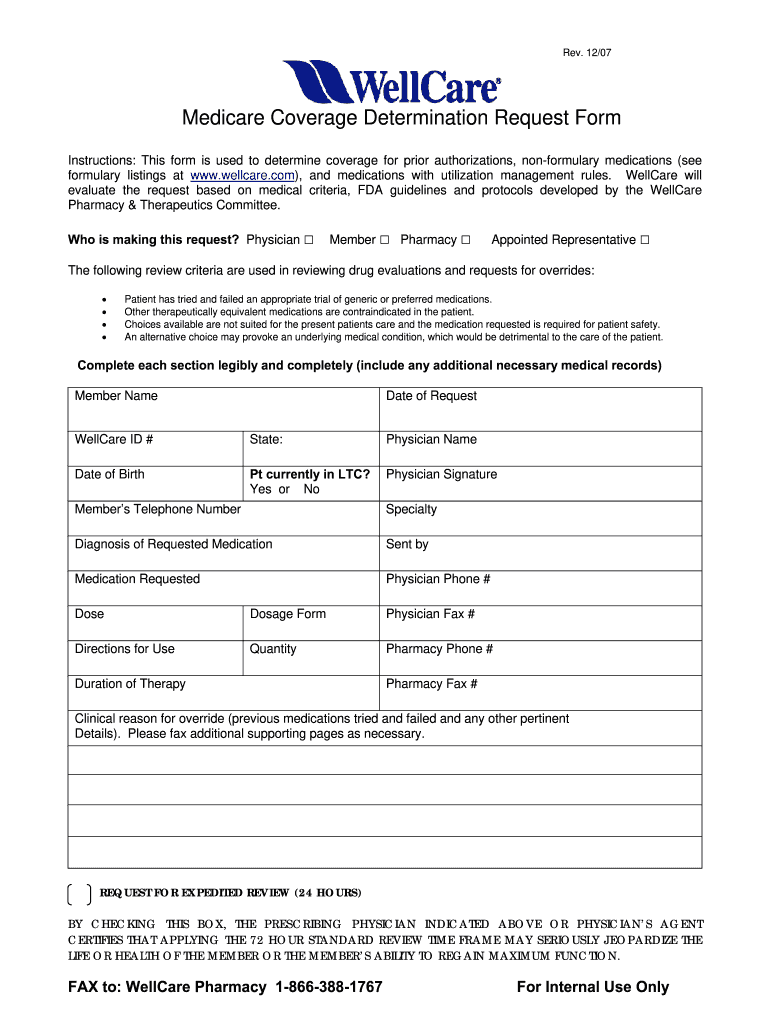
Free Wellcare Prior Prescription (Rx) Authorization Form PDF
Web request for redetermination of medicare prescription drug denial (appeal) (pdf) this form may be sent to us by mail or fax: (attach medical records for code audits, code edits or authorization denials. Contact us, or refer to the number on the back of your wellcare member id card. Prior authorization request form (pdf) inpatient fax cover letter (pdf) medication.
Wellcare Appeal Form Fill Online, Printable, Fillable, Blank pdfFiller
Contact us, or refer to the number on the back of your wellcare member id card. Access key forms for authorizations, claims, pharmacy and more. Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. An expedited redetermination (part d appeal) request can be made by phone at contact us or refer to.
Free Wellcare Prior Prescription (Rx) Authorization Form PDF
Providers may file a written appeal with the missouri care complaints and appeals department. Appeals should be addressed to: You can now quickly request an appeal for your drug coverage through the request for redetermination form. What is the procedure for filing an appeal? Contact us, or refer to the number on the back of your wellcare member id card.
WELLCARE HEALTH PLANS, INC. FORM 8K EX99.2 PRESENTATION DATED
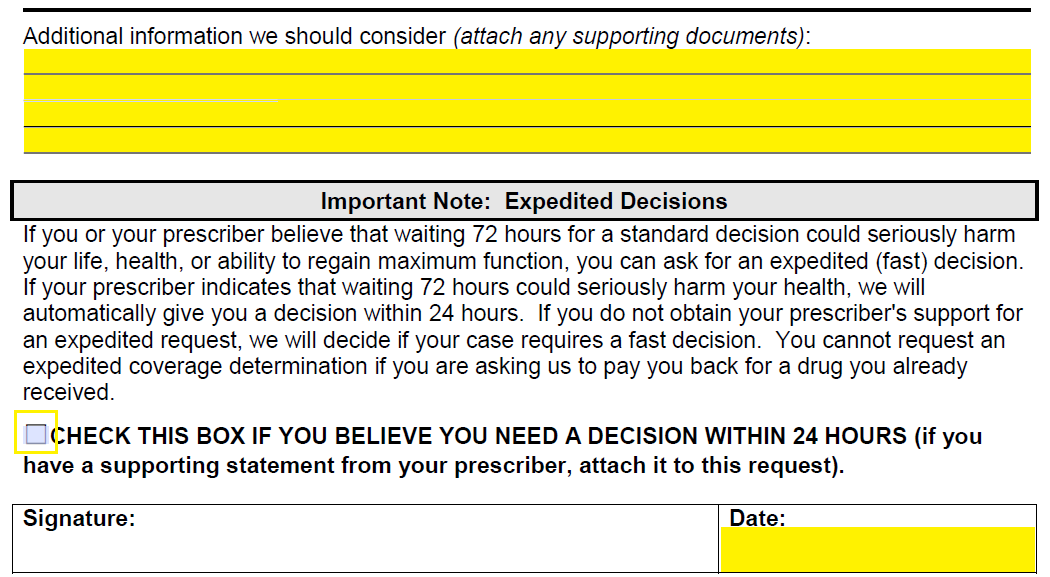
What is the procedure for filing an appeal? Complete an appeal of coverage determination request (pdf) and send it to: Web medication appeal request form you can use this form to request an appeal when a medication coverage determination request has been denied. Web request for redetermination of medicare prescription drug denial (appeal) (pdf) this form may be sent to.
Wellcare Forms For Prior Authorization Fill Out and Sign Printable
Web request for redetermination of medicare prescription drug denial (appeal) (pdf) this form may be sent to us by mail or fax: Prior authorization request form (pdf) inpatient fax cover letter (pdf) medication appeal request form (pdf) medicaid drug coverage request form (pdf) notice of pregnancy form (pdf) provider incident report form (pdf) pcp change request form for prepaid health.

Patient Portal Paloma Wellness and RehabPhysical Therapy
To access the form, please pick your state: An expedited redetermination (part d appeal) request can be made by phone at contact us or refer to the number on the back of your member id. Prior authorization request form (pdf) inpatient fax cover letter (pdf) medication appeal request form (pdf) medicaid drug coverage request form (pdf) notice of pregnancy form.

Fillable Online Ohio Provider Medical Prior Authorization Request Form
Do not attach original claim form.) Appeals 4205 philips farm road, suite 100 columbia, mo 65201. Please do not include this form with a corrected claim. Prior authorization request form (pdf) inpatient fax cover letter (pdf) medication appeal request form (pdf) medicaid drug coverage request form (pdf) notice of pregnancy form (pdf) provider incident report form (pdf) pcp change request.

Wellmed Prior Authorization Form Fill Online, Printable, Fillable
An expedited redetermination (part d appeal) request can be made by phone at contact us or refer to the number on the back of your member id. Complete an appeal of coverage determination request (pdf) and send it to: Web request for redetermination of medicare prescription drug denial (appeal) (pdf) this form may be sent to us by mail or.
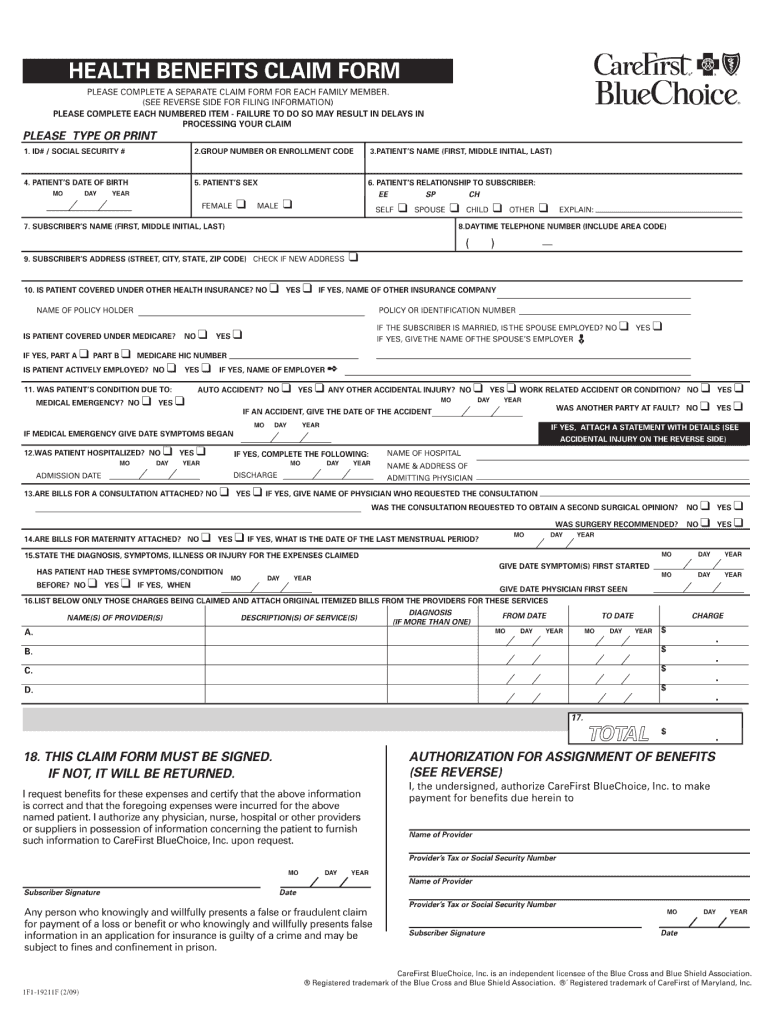
2009 Form CareFirst BlueChoice 1F119211F Fill Online, Printable
Missouri care health plan attn: Appeals 4205 philips farm road, suite 100 columbia, mo 65201. What is the procedure for filing an appeal? To access the form, please pick your state: Do not attach original claim form.)
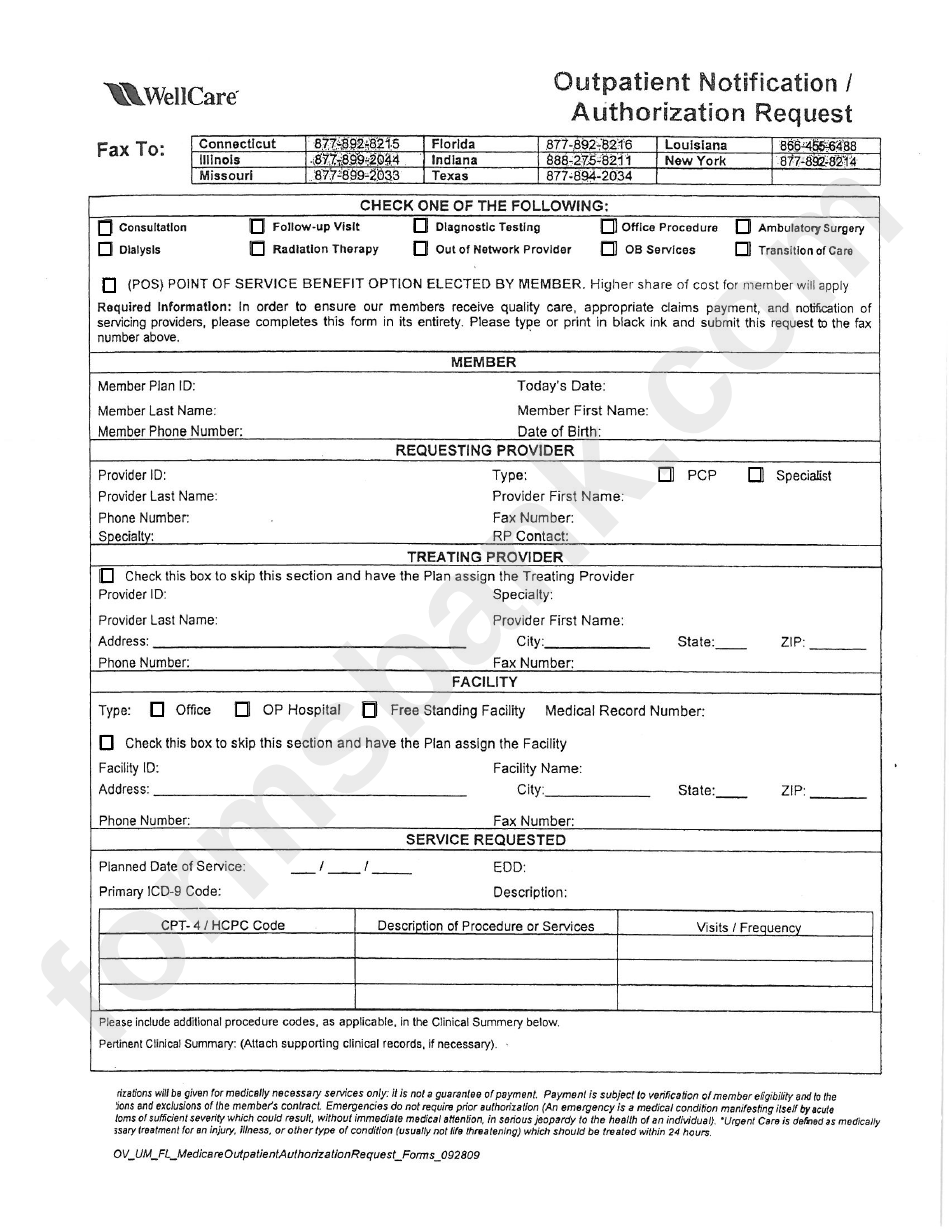
Fillable Outpatient Notification /authorization Request Wellcare
Missouri care health plan attn: What is the procedure for filing an appeal? Access key forms for authorizations, claims, pharmacy and more. Please do not include this form with a corrected claim. Web medication appeal request form you can use this form to request an appeal when a medication coverage determination request has been denied.
Access Key Forms For Authorizations, Claims, Pharmacy And More.
What is the procedure for filing an appeal? Contact us, or refer to the number on the back of your wellcare member id card. Web claim” process in the wellcare by allwell provider manual, found on superiorhealthplan.com/providermanuals. Web request for redetermination of medicare prescription drug denial (appeal) (pdf) this form may be sent to us by mail or fax:
Missouri Care Health Plan Attn:
Prior authorization request form (pdf) inpatient fax cover letter (pdf) medication appeal request form (pdf) medicaid drug coverage request form (pdf) notice of pregnancy form (pdf) provider incident report form (pdf) pcp change request form for prepaid health plans (phps) (pdf) We have redesigned our website. Web medication appeal request form you can use this form to request an appeal when a medication coverage determination request has been denied. You can now quickly request an appeal for your drug coverage through the request for redetermination form.
Appeals Should Be Addressed To:
(attach medical records for code audits, code edits or authorization denials. To access the form, please pick your state: Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. Appeals 4205 philips farm road, suite 100 columbia, mo 65201.
Wellcare, Medicare Pharmacy Appeals, P.o.
Complete an appeal of coverage determination request (pdf) and send it to: Providers may file a written appeal with the missouri care complaints and appeals department. Please do not include this form with a corrected claim. How long do i have to submit an appeal?