Free From Communicable Disease Form
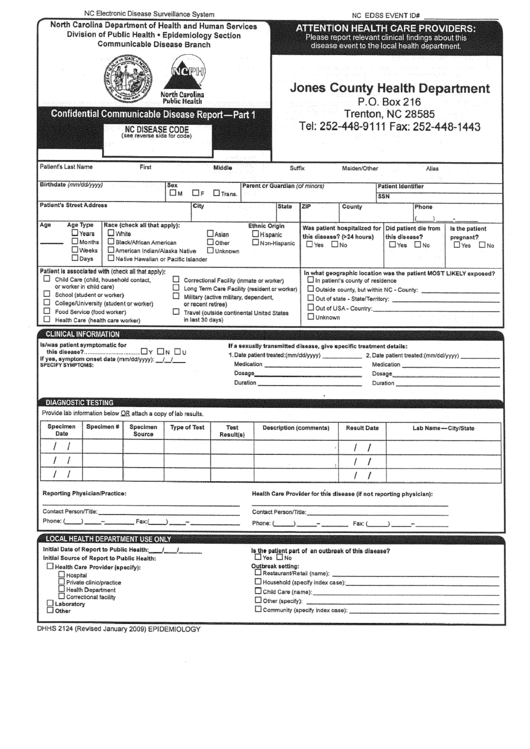
Free From Communicable Disease Form - Web statement of good health/free of communicable disease explanation and instruction: Web communicable disease report for healthcare providers. Tb screening inject date administered by. Signature of physician/physician’s assistant/nurse practitioner (circle one) date printed name of physician/physician’s assistant/nurse practitioner (circle one) Dates results diptheria, pertussis, tetanus (tdap) vaccine skin response to mantoux must be measured, recorded by a healthcare. Web the department requires that health care agencies or providers screen all health care staff within 90 days before direct contact and periodically, to ensure that staff is free of any communicable diseases before coming into contact with clients. Web communicable disease/physical form patient name:_____ date:_____ last first middle the following is required for nursing students: (to be completed by health care provider) _____ i have evaluated this individual and in my medical opinion, find him/her free from all communicable disease. He/she is in good physical and mental health, free of any communicable diseases and is able to function in his/her profession at full capacity. Absolute healthcare services, llc policy requires all employees who have direct contact with patients in the home setting to submit a statement from an appropriately licensed health care professional, based on an exam performed within the last twelve.
Web communicable disease report for healthcare providers. Web statement of good health/free of communicable disease explanation and instruction: Web to be completed by physician have examined the individual named above and to the best of my knowledge; Signature of physician/physician’s assistant/nurse practitioner (circle one) date printed name of physician/physician’s assistant/nurse practitioner (circle one) By signing below i certify that the above information is true. (to be completed by health care provider) _____ i have evaluated this individual and in my medical opinion, find him/her free from all communicable disease. He/she is in good physical and mental health, free of any communicable diseases and is able to function in his/her profession at full capacity. Web he/she is free of communicable diseases and is fit to work without restrictions or limitations. Dates results diptheria, pertussis, tetanus (tdap) vaccine skin response to mantoux must be measured, recorded by a healthcare. _____ i cannot at this time, ascertain that this individual is free of communicable disease.
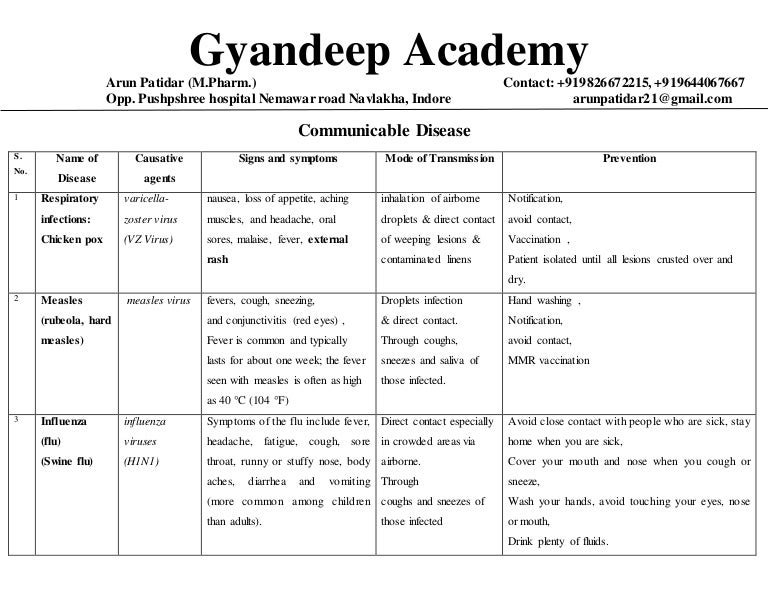
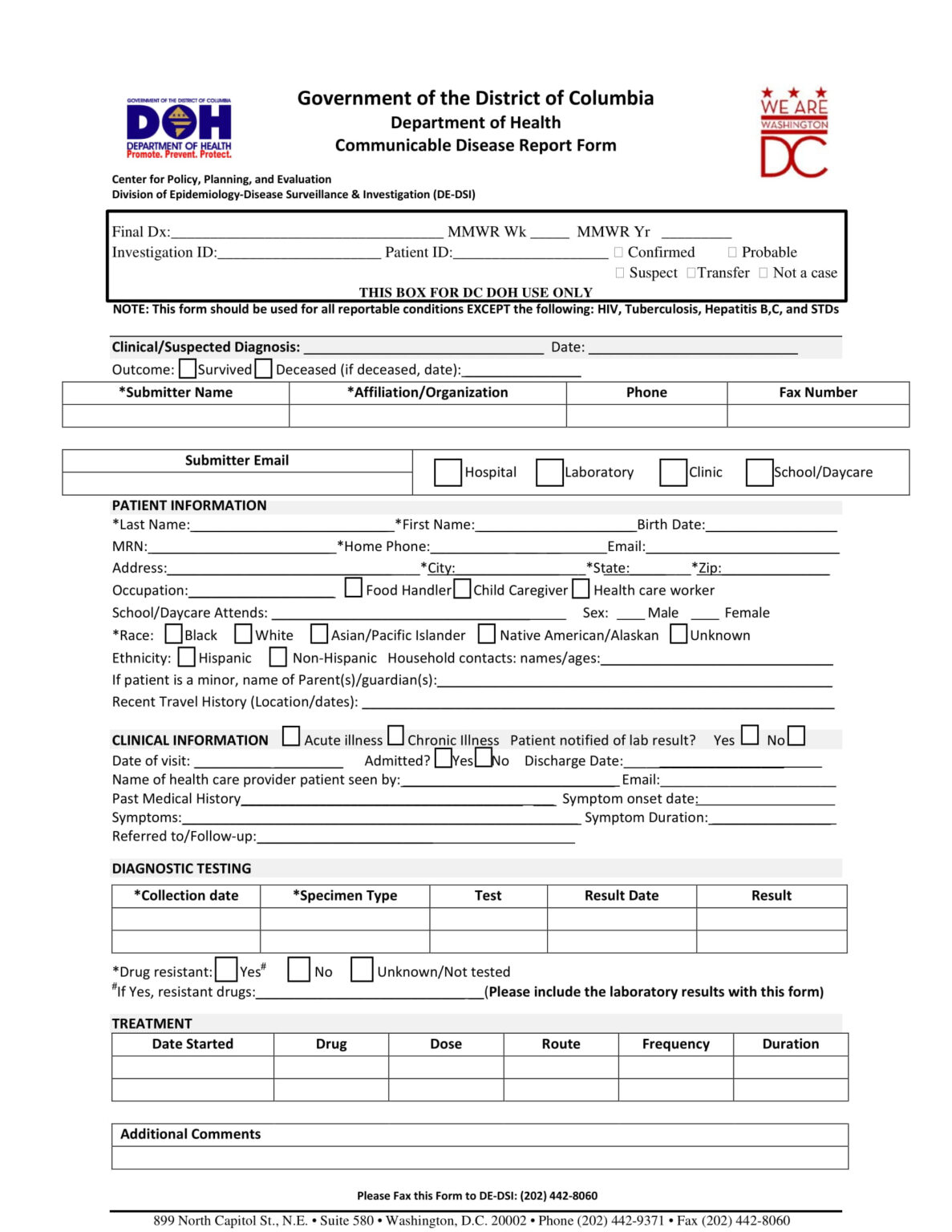
Web communicable disease report for healthcare providers. Dates results diptheria, pertussis, tetanus (tdap) vaccine skin response to mantoux must be measured, recorded by a healthcare. Communicable diseases, also known as infectious diseases or transmissible diseases, are illnesses that result from the infection, presence and growth of pathogenic (capable of causing disease) biologic agents in an individual human or other animal host. Web what is communicable disease in short form? Web to be completed by physician have examined the individual named above and to the best of my knowledge; Reporting is mandated for all diseases on the list unless otherwise indicated. Web communicable disease control forms infectious diseases case report forms (forms are provided for use by health professionals only) note: By signing below i certify that the above information is true. He/she is in good physical and mental health, free of any communicable diseases and is able to function in his/her profession at full capacity. _____ i cannot at this time, ascertain that this individual is free of communicable disease.
Communicable disease list
Web communicable disease report for healthcare providers. Web communicable disease/physical form patient name:_____ date:_____ last first middle the following is required for nursing students: Tb screening inject date administered by. Web communicable disease control forms infectious diseases case report forms (forms are provided for use by health professionals only) note: Web what is communicable disease in short form?

Fill Free fillable COMMUNICABLE DISEASE FORM FOR RABIES MATERIALS
(to be completed by health care provider) _____ i have evaluated this individual and in my medical opinion, find him/her free from all communicable disease. Web communicable disease/physical form patient name:_____ date:_____ last first middle the following is required for nursing students: Dates results diptheria, pertussis, tetanus (tdap) vaccine skin response to mantoux must be measured, recorded by a healthcare..
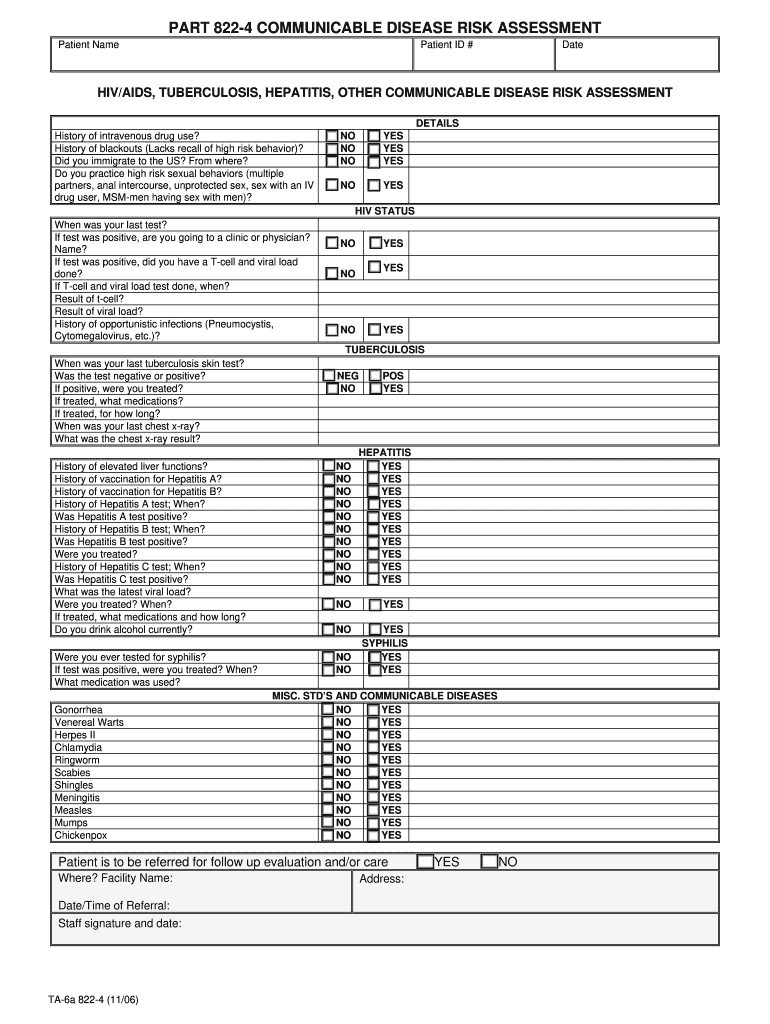
Oasas Communicable Disease Risk Assessmebr Part 822 4 Fill Online
Web the department requires that health care agencies or providers screen all health care staff within 90 days before direct contact and periodically, to ensure that staff is free of any communicable diseases before coming into contact with clients. Tb screening inject date administered by. Web to be completed by physician have examined the individual named above and to the.

I’m sick of disease Start now learning!
_____ i cannot at this time, ascertain that this individual is free of communicable disease. Web what is communicable disease in short form? Web statement of good health/free of communicable disease explanation and instruction: Web to be completed by physician have examined the individual named above and to the best of my knowledge; Web the department requires that health care.

Communicable Disease Report Resources Whole Child
Absolute healthcare services, llc policy requires all employees who have direct contact with patients in the home setting to submit a statement from an appropriately licensed health care professional, based on an exam performed within the last twelve. Web communicable disease/physical form patient name:_____ date:_____ last first middle the following is required for nursing students: Web to be completed by.
PPT Communicable Disease PowerPoint Presentation, free download ID
Dates results diptheria, pertussis, tetanus (tdap) vaccine skin response to mantoux must be measured, recorded by a healthcare. Web the department requires that health care agencies or providers screen all health care staff within 90 days before direct contact and periodically, to ensure that staff is free of any communicable diseases before coming into contact with clients. This form is.
Free 15+ Case Report Forms In Pdf Ms Word in Case Report Form
Dates results diptheria, pertussis, tetanus (tdap) vaccine skin response to mantoux must be measured, recorded by a healthcare. Web statement of good health/free of communicable disease explanation and instruction: Absolute healthcare services, llc policy requires all employees who have direct contact with patients in the home setting to submit a statement from an appropriately licensed health care professional, based on.
Communicable Disease Report Form For Healthcare Providers printable pdf
Web he/she is free of communicable diseases and is fit to work without restrictions or limitations. He/she is in good physical and mental health, free of any communicable diseases and is able to function in his/her profession at full capacity. Web what is communicable disease in short form? Tb screening inject date administered by. Communicable diseases, also known as infectious.

PPT Communicable Disease PowerPoint Presentation, free download ID
Tb screening inject date administered by. By signing below i certify that the above information is true. Web statement of good health/free of communicable disease explanation and instruction: Web communicable disease report for healthcare providers. _____ i cannot at this time, ascertain that this individual is free of communicable disease.
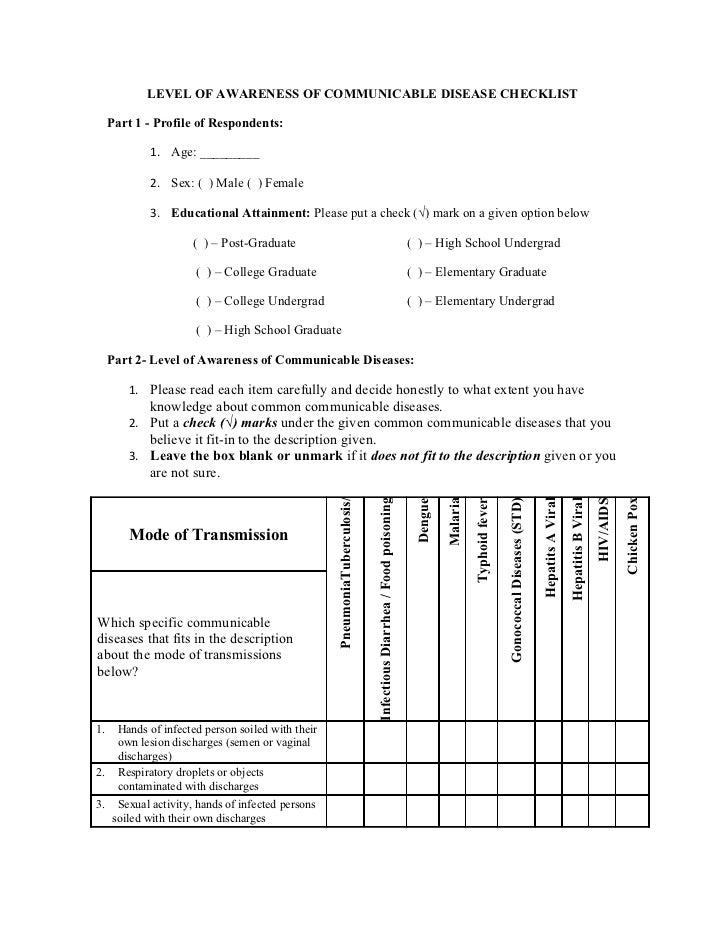
Level of awareness of communicable disease checklist
_____ i cannot at this time, ascertain that this individual is free of communicable disease. (to be completed by health care provider) _____ i have evaluated this individual and in my medical opinion, find him/her free from all communicable disease. Reporting is mandated for all diseases on the list unless otherwise indicated. He/she is in good physical and mental health,.
He/She Is In Good Physical And Mental Health, Free Of Any Communicable Diseases And Is Able To Function In His/Her Profession At Full Capacity.
Reporting is mandated for all diseases on the list unless otherwise indicated. _____ i cannot at this time, ascertain that this individual is free of communicable disease. Dates results diptheria, pertussis, tetanus (tdap) vaccine skin response to mantoux must be measured, recorded by a healthcare. Signature of physician/physician’s assistant/nurse practitioner (circle one) date printed name of physician/physician’s assistant/nurse practitioner (circle one)
Web He/She Is Free Of Communicable Diseases And Is Fit To Work Without Restrictions Or Limitations.
Web the department requires that health care agencies or providers screen all health care staff within 90 days before direct contact and periodically, to ensure that staff is free of any communicable diseases before coming into contact with clients. Tb screening inject date administered by. Web communicable disease/physical form patient name:_____ date:_____ last first middle the following is required for nursing students: This form is intended to provide guidance for providers.
Web Communicable Disease Control Forms Infectious Diseases Case Report Forms (Forms Are Provided For Use By Health Professionals Only) Note:
Web statement of good health/free of communicable disease explanation and instruction: Communicable diseases, also known as infectious diseases or transmissible diseases, are illnesses that result from the infection, presence and growth of pathogenic (capable of causing disease) biologic agents in an individual human or other animal host. By signing below i certify that the above information is true. Web what is communicable disease in short form?
(To Be Completed By Health Care Provider) _____ I Have Evaluated This Individual And In My Medical Opinion, Find Him/Her Free From All Communicable Disease.
Absolute healthcare services, llc policy requires all employees who have direct contact with patients in the home setting to submit a statement from an appropriately licensed health care professional, based on an exam performed within the last twelve. Web communicable disease report for healthcare providers. Web to be completed by physician have examined the individual named above and to the best of my knowledge;