Eyemed In Network Claim Form
Eyemed In Network Claim Form - Web the cigna vision network. Return the completed form and your. Web eyemed out of network claim form. Web claim form out of network vision claim form let's get started! You only need to complete this form if you are visiting a. Web welcome to the online claims processing system. Use our enhanced provider search. You only need to complete this. Doctor or store information name street address city state zip. Online click below to complete an electronic claim form.
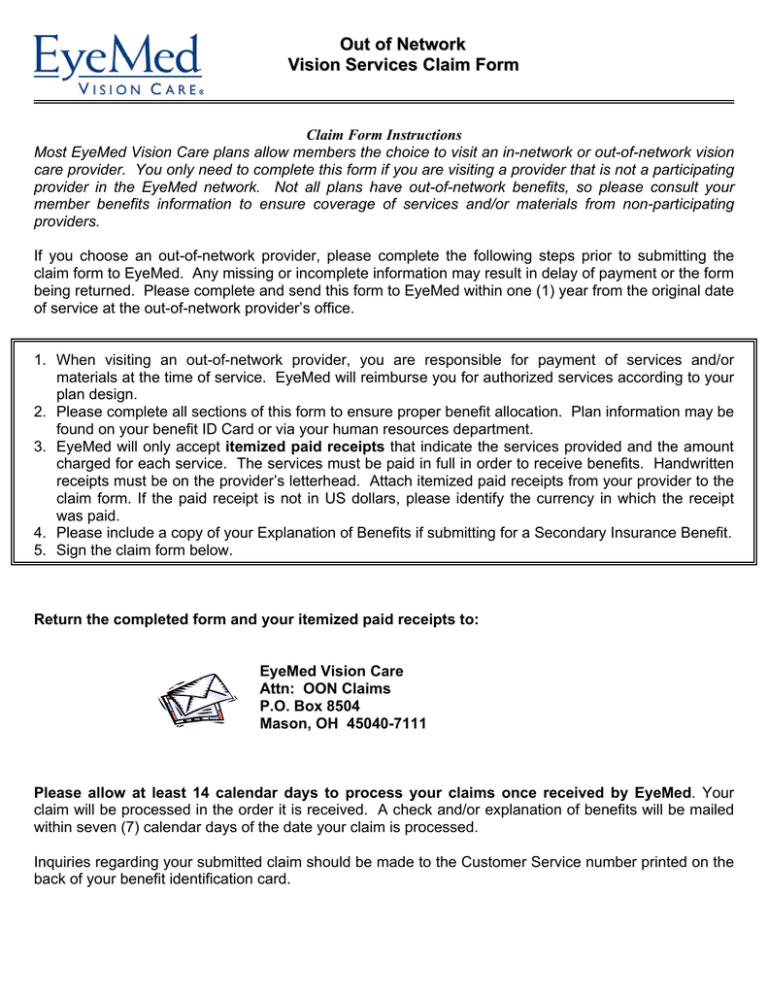
Return the completed form and your. You only need to complete this form if you are visiting a. Need to access resources on infocus? Use our enhanced provider search. Online click below to complete an electronic claim form. Web you can now submit your form online or by mail: If the paid receipt is not in us dollars, please identify the currency in which the receipt was paid. One of the following exceptions must apply, based on your home or. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24. Claim form, vision, vision certificate.
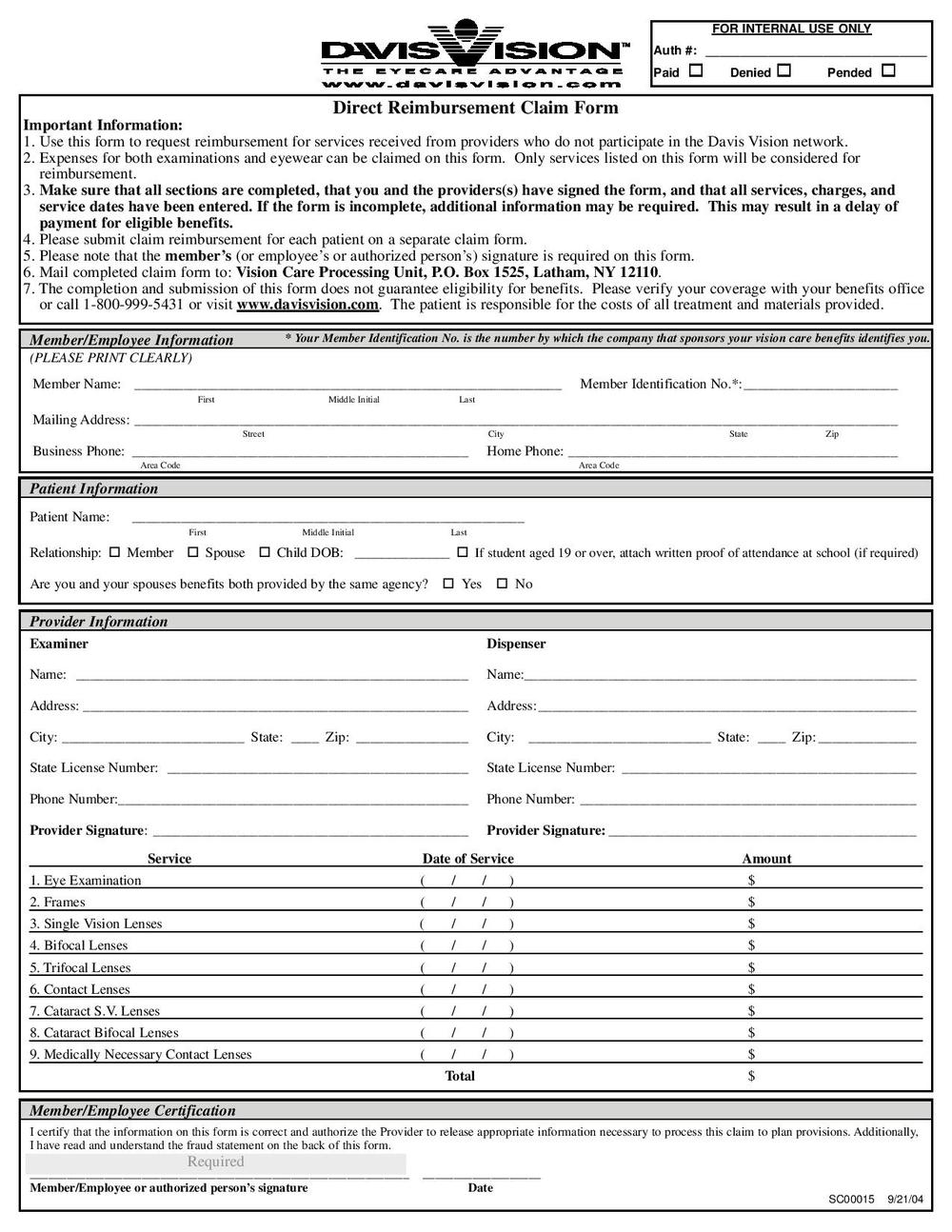
You only need to complete this form if you are visiting a. Web out of network/indemnity vision services claim form claim form instructions to request reimbursement, please complete and sign the itemized claim. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24. Claim form, vision, vision certificate. Return the completed form and your. Web welcome to the online claims processing system. Need to access resources on infocus? One of the following exceptions must apply, based on your home or. You can now submit your form online or. If the paid receipt is not in us dollars, please identify the currency in which the receipt was paid.

Eyemed Insurance Out Of Network Claim Form Creativmakeup Co
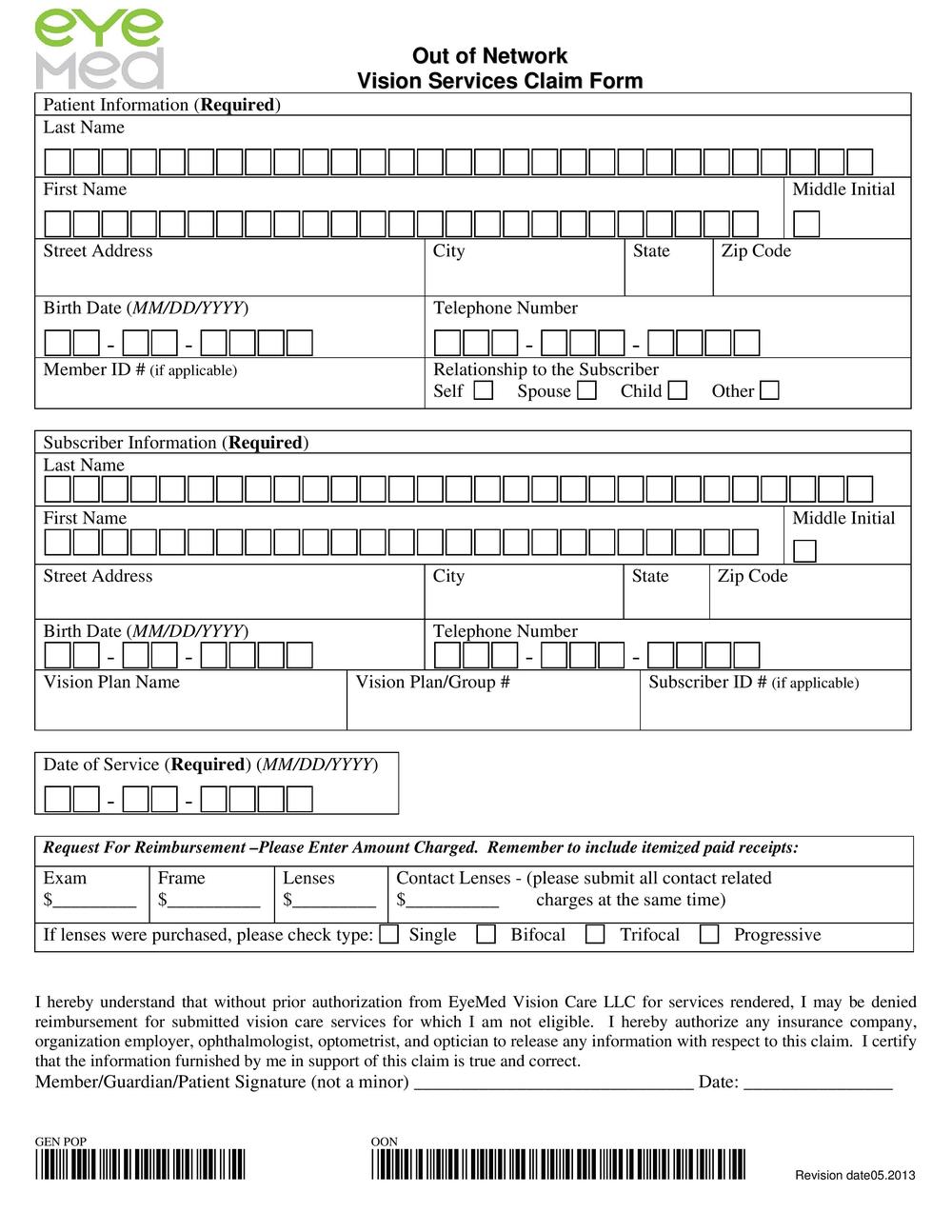
To submit a claim please enter your email address below and we'll email you a link that will only be active for 24. Claim form, vision, vision certificate. Need to access resources on infocus? Patient and subscriber information last name first name date of birth street address city state zip code 2. Online click below to complete an electronic claim.
Drs. Robert Stahl & Amy Calder, Optometrists Blog
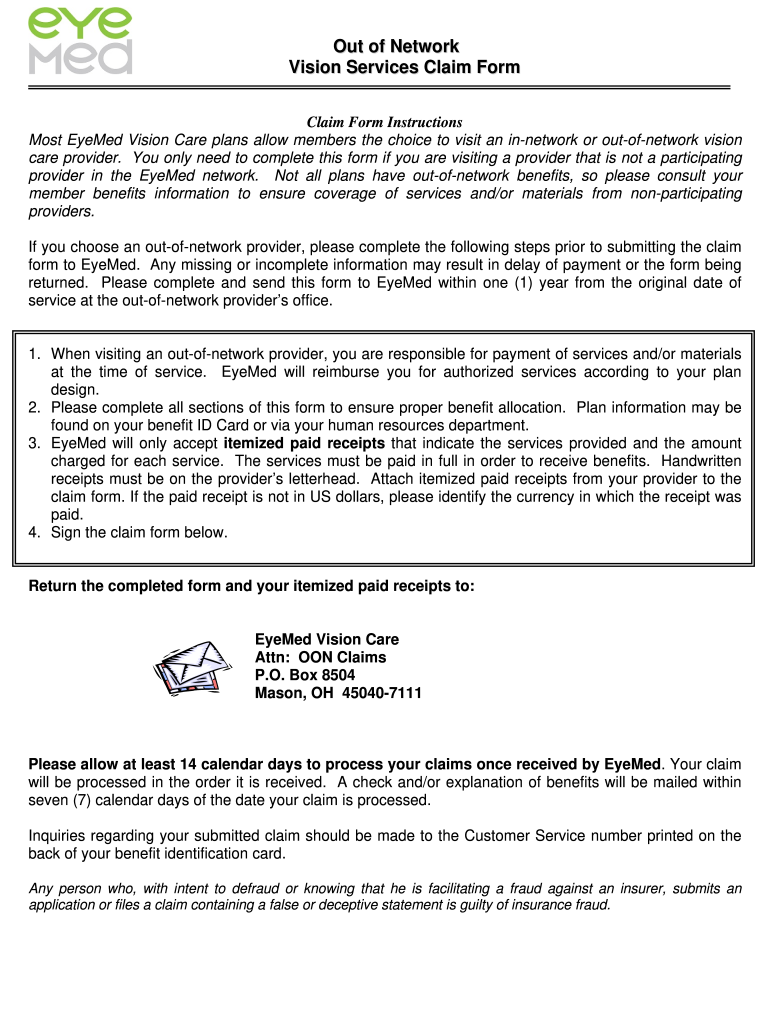
Sign the claim form below. Doctor or store information name street address city state zip. Web eyemed out of network claim form. Web welcome to the online claims processing system. To request account access, complete our online registration form.
O u t
One of the following exceptions must apply, based on your home or. Web eyemed out of network claim form. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24. Web claim form out of network vision claim form let's get started! Web you can now submit your.
OH EyeMed Claim Form Fill and Sign Printable Template Online US
Web welcome to the online claims processing system. Return the completed form and your. Go green and get paid faster. Online click below to complete an electronic claim form. One of the following exceptions must apply, based on your home or.
Drs. Robert Stahl & Amy Calder, Optometrists Blog
You only need to complete this form if you are visiting a. Patient and subscriber information last name first name date of birth street address city state zip code 2. To request account access, complete our online registration form. Return the completed form and your. Go green and get paid faster.

Eye Exam forms Template Luxury Eye Examination form Pdf Exam, Eye
Return the completed form and your. One of the following exceptions must apply, based on your home or. Claim form, vision, vision certificate. If the paid receipt is not in us dollars, please identify the currency in which the receipt was paid. Web you can now submit your form online or by mail:

Vision Insurance in Denver EyeMed Health First Optical Masters
To submit a claim please enter your email address below and we'll email you a link that will only be active for 24. You only need to complete this. Patient and subscriber information last name first name date of birth street address city state zip code 2. Web the cigna vision network. Claim form, vision, vision certificate.

Eyemed Claim Form Printable
You only need to complete this. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24. Online click below to complete an electronic claim form. Doctor or store information name street address city state zip. If the paid receipt is not in us dollars, please identify the.
List of Providers For EyeMed Pocket Sense
If the paid receipt is not in us dollars, please identify the currency in which the receipt was paid. Web eyemed out of network claim form. To request account access, complete our online registration form. Doctor or store information name street address city state zip. Web you can now submit your form online or by mail:

Optometry in Gardena Stahl and Calder
Return the completed form and your. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24. If the paid receipt is not in us dollars, please identify the currency in which the receipt was paid. Sign the claim form below. Web you can now submit your form.
Web Eyemed Out Of Network Claim Form.
Web welcome to the online claims processing system. Go green and get paid faster. Web you can now submit your form online or by mail: If the paid receipt is not in us dollars, please identify the currency in which the receipt was paid.
Web Out Of Network/Indemnity Vision Services Claim Form Claim Form Instructions To Request Reimbursement, Please Complete And Sign The Itemized Claim.
You can now submit your form online or. One of the following exceptions must apply, based on your home or. Need to access resources on infocus? Doctor or store information name street address city state zip.
Return The Completed Form And Your.
To request account access, complete our online registration form. Claim form, vision, vision certificate. You only need to complete this. Online click below to complete an electronic claim form.
Patient And Subscriber Information Last Name First Name Date Of Birth Street Address City State Zip Code 2.
You only need to complete this form if you are visiting a. Sign the claim form below. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24. Web the cigna vision network.