Dwc-1 Claim Form
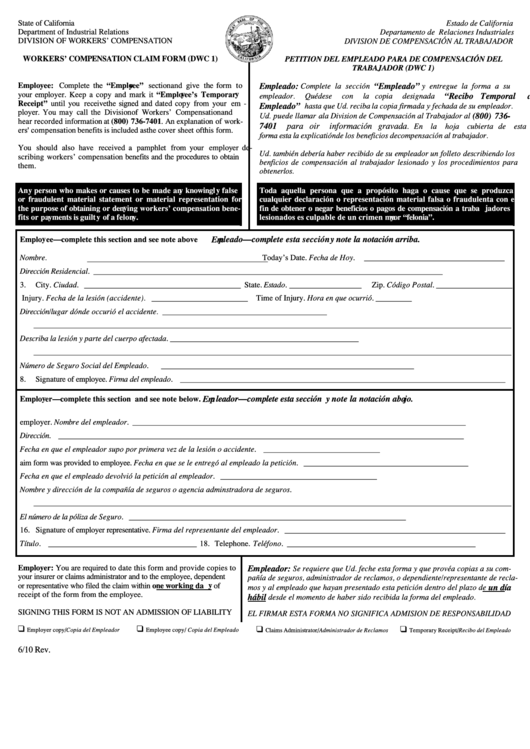
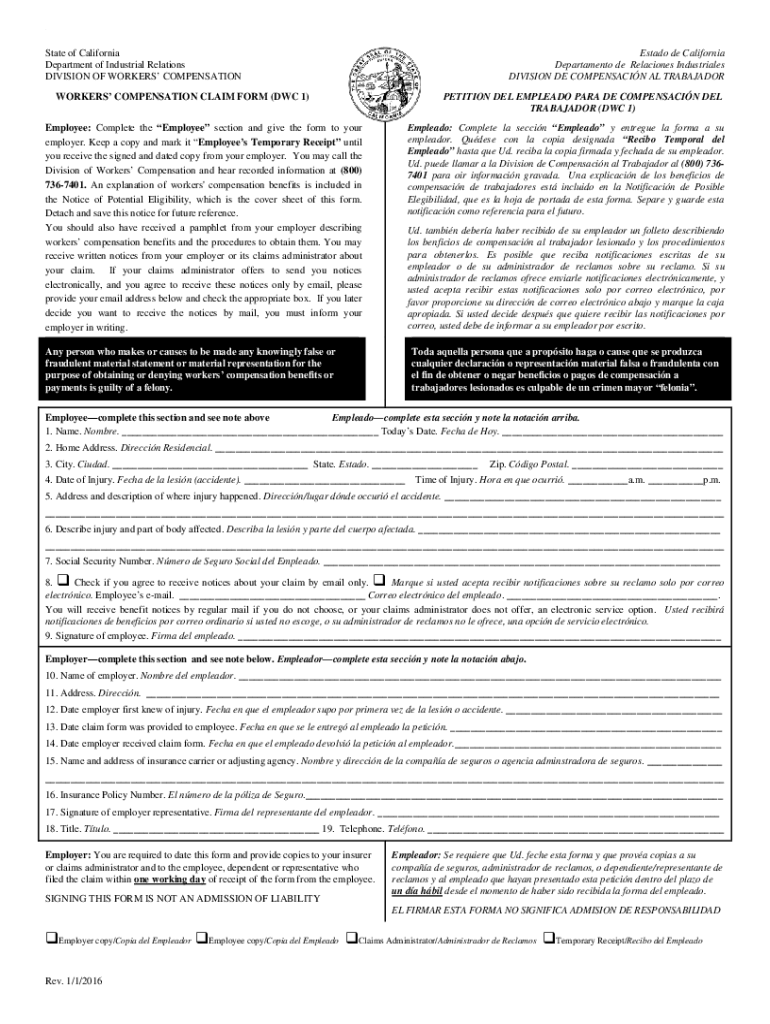
Dwc-1 Claim Form - Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. Details of the claimant's employment and circumstances surrounding the injury or illness are also requested. If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting from a workplace crime, you may be entitled to workers’ compensation benefits. Medical mileage expense form english/spanish * for travel on or after 1/1/23 How to file a workers' compensation claim form. Use the attached form to file a workers’ compensation claim with your employer. Claim form (dwc 1) note: How to request a qualified medical evaluation. Required checklist for filing this form (please file the forms in the order indicated) In california, injured workers are entitled to benefits, such as temporary disability, permanent disability and medical treatment.
Sections 133, 5307.3 and 5401, labor code. Details of the claimant's employment and circumstances surrounding the injury or illness are also requested. Name and title of person comple ting form claims coordinator 41. Workplace injuries can happen at any time to anyone. Medical mileage expense form english/spanish * for travel on or after 1/1/23 Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. Agency mailing address and telephone number Web how to fill out a claim form. If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting from a workplace crime, you may be entitled to workers’ compensation benefits. Use the attached form to file a workers’ compensation claim with your employer.
Agency mailing address and telephone number Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. Use the attached form to file a workers’ compensation claim with your employer. Workplace injuries can happen at any time to anyone. Name (please leave blank spaces between numbers, names or words) Therefore, it's important to know what to do if you are hurt at work. Complete only the “employee” section of the form and send it to your employer right away. 1/1/2016 page 1 of 3. 10/05) page 1 division of workers’ compensation 1. You should read all of the information.
Form DFSF2DWC49 Download Fillable PDF or Fill Online Aggregate
Name and title of person comple ting form claims coordinator 41. Be sure to sign and date the claim form and keep a copy for your records. How to request a qualified medical evaluation. If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting from a workplace crime, you may be entitled.
Form DWC EDI03 Download Fillable PDF or Fill Online Medical Edi
Required checklist for filing this form (please file the forms in the order indicated) 1/1/2016 page 1 of 3. Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. Workers' compensation claim form (dwc 1) and notice of potential eligibility. You should read all of.
DWCAD Form 101 Download Fillable PDF or Fill Online Request for
Workplace injuries can happen at any time to anyone. Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. Details of the claimant's employment and circumstances surrounding the injury or illness are also requested. 10/05) page 1 division of workers’ compensation 1. How to request.

Gallery of Workers Compensation form Dwc 1 Inspirational Claim form
1/1/2016 page 1 of 3. Sections 132(a), 139.48, 139.6, 4600, 4600.3, 4601, 4604.5, 4616, 4650, 4656, 4658.5, 4658.6, 4700, 4701, 4702, 4703, 5400, 5401, 5401.7 and 5402,. Agency mailing address and telephone number Name (please leave blank spaces between numbers, names or words) Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and.
Workers’ Compensation Claim Form (DWC 1) & Notice of Potential
Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting from a workplace crime, you may be entitled to workers’ compensation benefits. Return the claim form to.
Form Dwc 1 Workers' Compensation Claim Form printable pdf download
Name (please leave blank spaces between numbers, names or words) Claim form (dwc 1) note: 10/05) page 1 division of workers’ compensation 1. Therefore, it's important to know what to do if you are hurt at work. Complete only the “employee” section of the form and send it to your employer right away.

Dwc 1 Fill Online, Printable, Fillable, Blank PDFfiller Filling
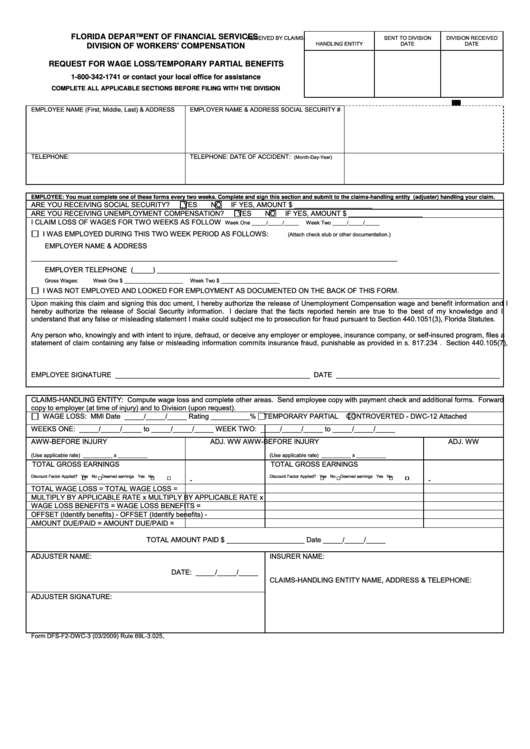
Medical mileage expense form english/spanish * for travel on or after 1/1/23 Name and title of person comple ting form claims coordinator 41. Web workers' compensation claim form. Web how to fill out a claim form. How to file a workers' compensation claim form.

DWC 1 Form In the heights, Lift and carry, Compensation claim
Name (please leave blank spaces between numbers, names or words) Medical mileage expense form english/spanish * for travel on or after 1/1/23 Use the attached form to file a workers’ compensation claim with your employer. If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting from a workplace crime, you may be.
Dwc 1 Claim Form mekabdesigns
Use the attached form to file a workers’ compensation claim with your employer. Agency mailing address and telephone number Required checklist for filing this form (please file the forms in the order indicated) Details of the claimant's employment and circumstances surrounding the injury or illness are also requested. Name (please leave blank spaces between numbers, names or words)
20162021 Form CA DIR DWC 1 Fill Online, Printable, Fillable, Blank
Be sure to sign and date the claim form and keep a copy for your records. Name (last, first, m.i.) 2. Medical mileage expense form english/spanish * for travel on or after 1/1/23 Claim form (dwc 1) note: Use the attached form to file a workers’ compensation claim with your employer.
Web Workers' Compensation Claim Form.
Medical mileage expense form english/spanish * for travel on or after 1/1/23 Be sure to sign and date the claim form and keep a copy for your records. How to request a qualified medical evaluation. If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting from a workplace crime, you may be entitled to workers’ compensation benefits.
10/05) Page 1 Division Of Workers’ Compensation 1.
Use the attached form to file a workers’ compensation claim with your employer. Details of the claimant's employment and circumstances surrounding the injury or illness are also requested. You should read all of the information. How to file a workers' compensation claim form.
Web How To Fill Out A Claim Form.
Therefore, it's important to know what to do if you are hurt at work. Workers' compensation claim form (dwc 1) and notice of potential eligibility. Return the claim form to your employer in person or by mail. 1/1/2016 page 1 of 3.
Web Formulario De Reclamo De Compensación De Trabajadores (Dwc 1) Y Notificación De Posible Elegibilidad If You Are Injured Or Become Ill, Either Physically Or Mentally, Because Of Your Job, Including Injuries Resulting From A Workplace Crime, You May Be Entitled To Workers’ Compensation Benefits.
Name (please leave blank spaces between numbers, names or words) Required checklist for filing this form (please file the forms in the order indicated) Complete only the “employee” section of the form and send it to your employer right away. Name and title of person comple ting form claims coordinator 41.