Doh Form For Home Care
Doh Form For Home Care - I also understand that this physician’s order is subject to the new york state department of health regulations at part 515, 516, 517, and 518 of title 18 nycrr, which permit the department to impose monetary penalties on, or. Verbal start of care and nurse's signature and date where applicable: Web legislative changes to the home care aide profession. Assistance with instrumental activities of daily living. This form also outlines what, and with whom, health information can be shared. Web need a blank doh form? Below you can get an idea about how to edit and complete a doh form in detail. You must choose at least two home health services in order to have an approved home health service category. Expanded syringe access program (esap) forms. Please check all that apply.
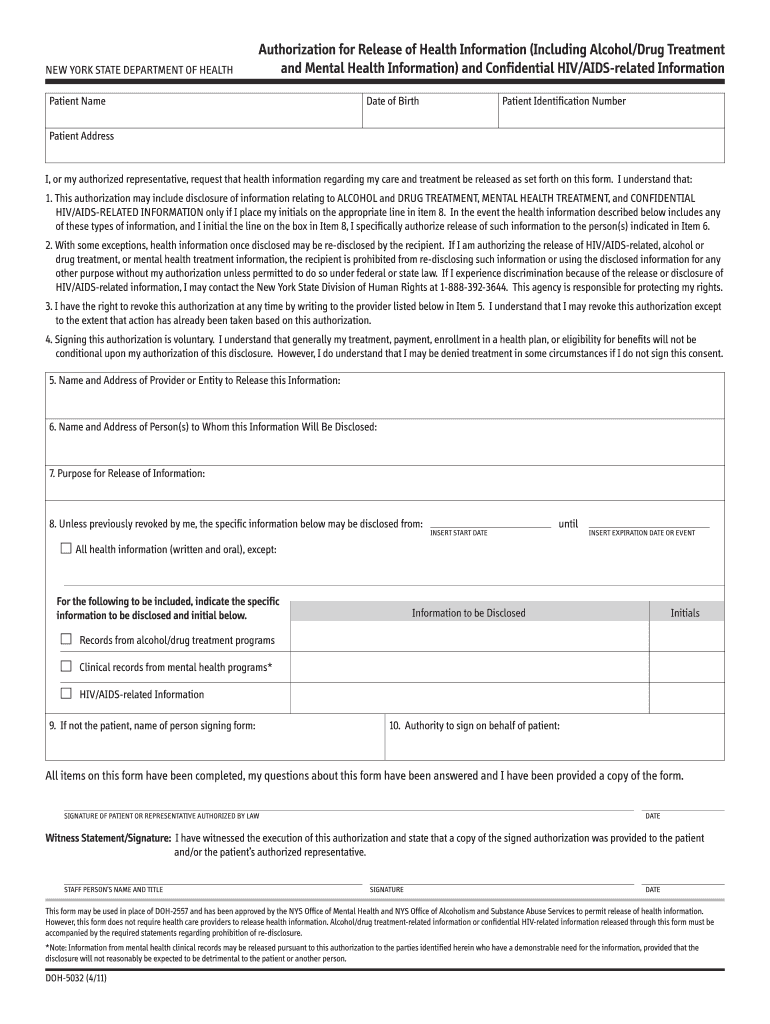
Web this form must be used for children less than 18 years of age for enrollment in a health home. Pick a tool you require from the toolbar that pops up in the dashboard. You must choose at least two home health services in order to have an approved home health service category. Web legislative changes to the home care aide profession. Pool or spa accident/injury report. Web home care ai485 home health certification and plan of treatment 23. You will simply complete the required forms and pay the fee. I also understand that this physician’s order is subject to the new york state department of health regulations at part 515, 516, 517, and 518 of title 18 nycrr, which permit the department to impose monetary penalties on, or. Pool fecal accident response form. Below you can get an idea about how to edit and complete a doh form in detail.
If the extension request is approved by doh, the new due date will be. Web licenses, permits, & certificates. Web requirements for home care aide certification 1. Verbal start of care and nurse's signature and date where applicable: The child does not meet the specified age requirement (age 10 or 12 ); An entity operating as a licensed home health agency must offer two skilled services on an intermittent basis, one of which must be skilled nursing. Submit the completed home care aide application to the department of health, including the employment verification form. This form also outlines what, and with whom, health information can be shared. Outdoor smoker, grill, or bbq unit permit application. Web home care ai485 home health certification and plan of treatment 23.
Form DOH5178AIT Supplement A Download Printable PDF or Fill Online
Physician's name and address 25. Of social services in connection with my request for home care. Here you would be transferred into a splasher allowing you to conduct edits on the document. Pool or spa accident/injury report. I also understand that this physician’s order is subject to the new york state department of health regulations at part 515, 516, 517,.
Form DOH1056C Schedule 1 Download Fillable PDF or Fill Online
Web president joe biden on tuesday announced new action to guarantee access to mental health care, unveiling a proposed rule that would ensure mental health benefits on private insurance plans more. Parent/guardian permission acknowledgement for vaccinations. Please check all that apply. Web recommend the number of hours of personal care services this patient may require. Please check all that apply.

Doh 1013 Form Fill Online, Printable, Fillable, Blank pdfFiller
Web mobile unit food permit application. Assistance with instrumental activities of daily living. An entity operating as a licensed home health agency must offer two skilled services on an intermittent basis, one of which must be skilled nursing. Parent/guardian permission acknowledgement for vaccinations. Web home health state licensure forms and resources.
Doh Application Form 2019 Fill Out and Sign Printable PDF Template
Hiv/aids educational materials order forms. You will simply complete the required forms and pay the fee. Web treatment to the new york city hra/ dept. Web home health state licensure forms and resources. Web mobile unit food permit application.
Form DOH4346 Download Printable PDF or Fill Online Specific Waiver
Web legislative changes to the home care aide profession. Verbal start of care and nurse's signature and date where applicable: Web recommend the number of hours of personal care services this patient may require. Physician's name and address 25. Web mobile unit food permit application.
Doh 5203 Fill Out and Sign Printable PDF Template signNow
I also understand that this physician’s order is subject to the new york state department of health regulations at part 515, 516, 517, and 518 of title 18 nycrr, which permit the department to impose monetary penalties on, or. If a home care aide credential is expired less than five years, no continuing education is required to renew the credential..

NY DOH Form LDSS3139 19792021 Fill and Sign Printable Template
Web licenses, permits, & certificates. Submit the completed home care aide application to the department of health, including the employment verification form. Permission is denied by the child’s parent/guardian/legally authorized representative to meeting alone with the child; This form also outlines what, and with whom, health information can be shared. Web legislative changes to the home care aide profession.
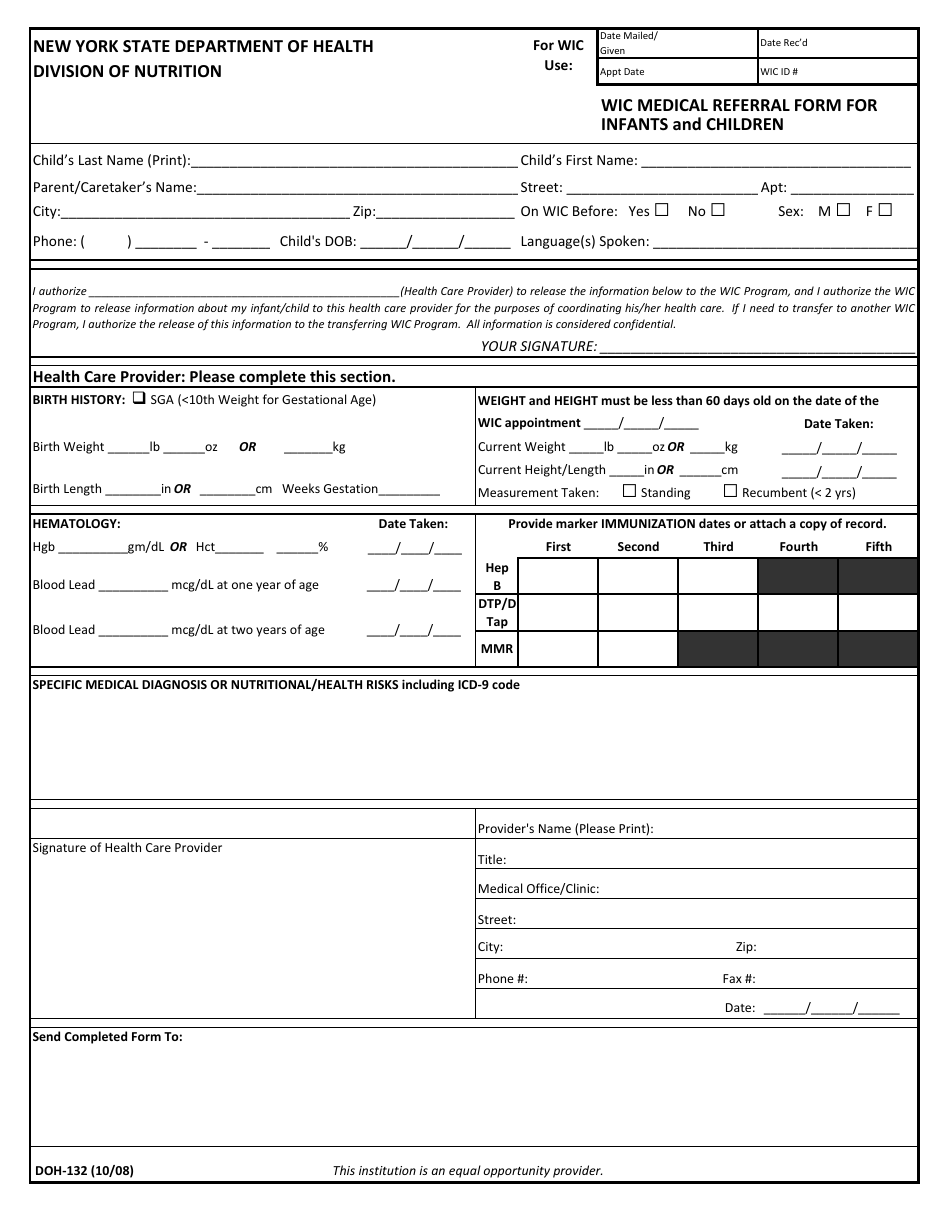
Form DOH132 Download Printable PDF or Fill Online Wic Medical Referral
Web this form must be used for children less than 18 years of age for enrollment in a health home. Web president joe biden on tuesday announced new action to guarantee access to mental health care, unveiling a proposed rule that would ensure mental health benefits on private insurance plans more. Due to recent legislation, the following changes take place.
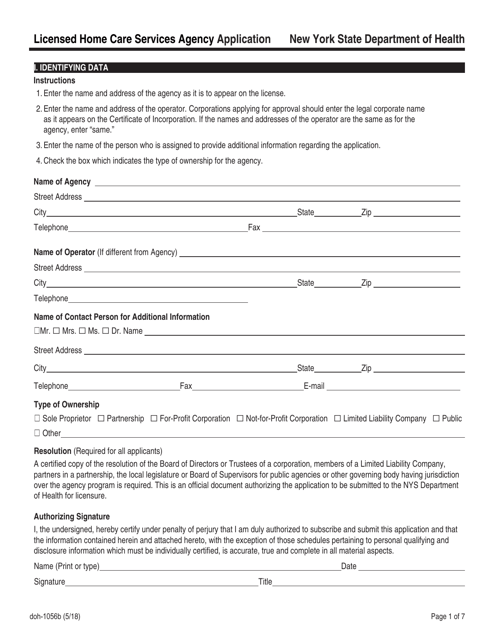
Form DOH1056B Download Fillable PDF or Fill Online Licensed Home Care
Of social services in connection with my request for home care. Submit the completed home care aide application to the department of health, including the employment verification form. Web mobile unit food permit application. An entity operating as a licensed home health agency must offer two skilled services on an intermittent basis, one of which must be skilled nursing. Verbal.
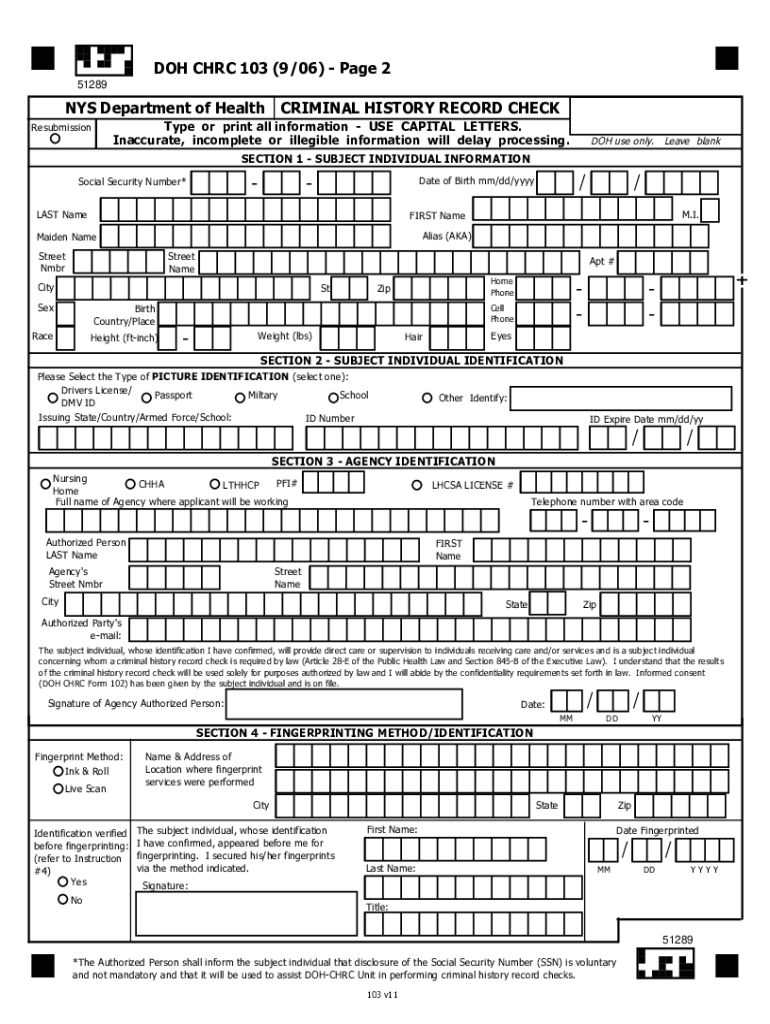
Form Chrc Fill Out and Sign Printable PDF Template signNow
Web need a blank doh form? Submit the completed home care aide application to the department of health, including the employment verification form. Physician's name and address 25. The information reported on the form includes the patient's name, address, date of admission, date of discharge (if applicable), type of payment source, diagnosis codes, and the care and services. Below you.
Web President Joe Biden On Tuesday Announced New Action To Guarantee Access To Mental Health Care, Unveiling A Proposed Rule That Would Ensure Mental Health Benefits On Private Insurance Plans More.
Web recommend the number of hours of personal care services this patient may require. Web home care ai485 home health certification and plan of treatment 23. Web licenses, permits, & certificates. Web requirements for home care aide certification 1.
Web A Comprehensive Guide To Editing The Doh Form.
Pool or spa accident/injury report. Please check all that apply. Please check all that apply. Push the“get form” button below.
You Must Choose At Least Two Home Health Services In Order To Have An Approved Home Health Service Category.
Web watch newsmax live for the latest news and analysis on today's top stories, right here on facebook. Outdoor smoker, grill, or bbq unit permit application. Of social services in connection with my request for home care. Web this form must be used for children less than 18 years of age for enrollment in a health home.
Submit The Completed Home Care Aide Application To The Department Of Health, Including The Employment Verification Form.
I also understand that this physician’s order is subject to the new york state department of health regulations at part 515, 516, 517, and 518 of title 18 nycrr, which permit the department to impose monetary penalties on, or. Assistance with instrumental activities of daily living. Web legislative changes to the home care aide profession. Verbal start of care and nurse's signature and date where applicable: