Cigna Wellness Screening Form
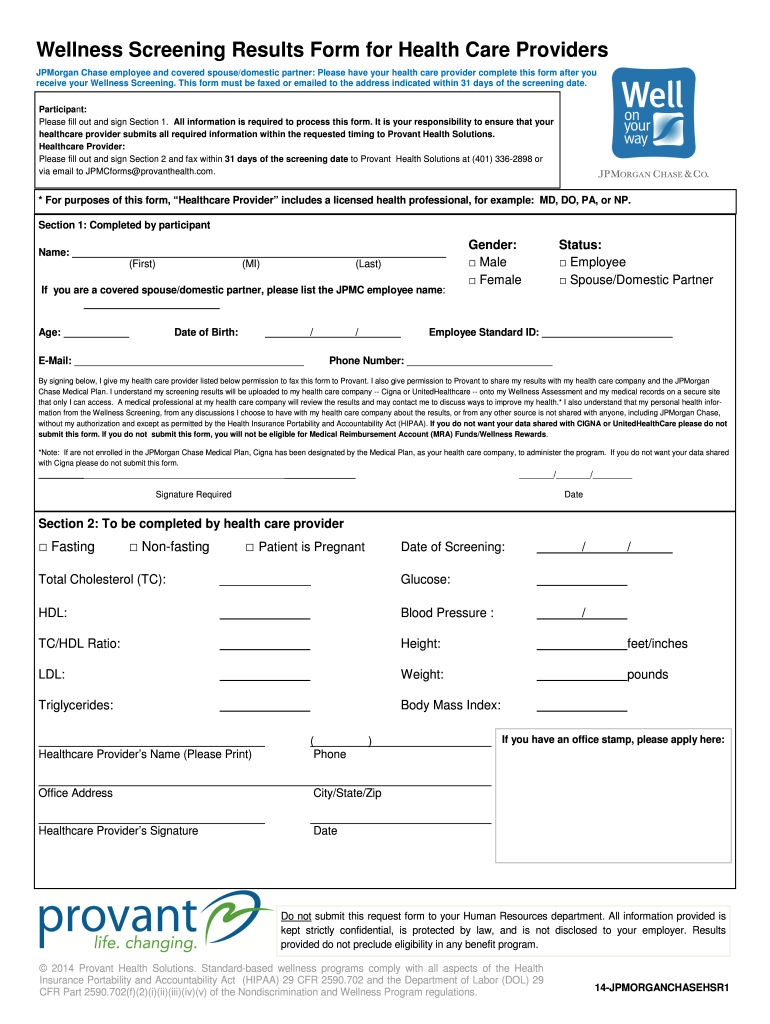
Cigna Wellness Screening Form - Please submit your claim through new york life. Accidental injury claim form [pdf] critical illness claim form [pdf] hospital care claim form [pdf] wellness incentive claim form [pdf] life, ad&d, or disability claims. Complete the mycigna online health assessment (250 wellness points) step 2: Residence pcp office facility telehealth (audiovisual only) 360 annual wellness examother source patient other (name & relationship) sex at birth: New york paid family leave forms Web annual physical exam/wellness screening form harris health system employees and spouses now have the option to use this custom wellness screening form to receive credit for their annual physical exams and biometric values on www.mycigna.com. Forms without a signature and date are incomplete. Submit your support id is: Web how to file a claim for wellness incentive benefits cigna accidental injury insurance your cigna accidental injury insurance plan comes with a wellness incentive benefit. Earn at least 500 additional wellness points through programs and activities (750 total wellness points)
Web annual physical exam/wellness screening form harris health system employees and spouses now have the option to use this custom wellness screening form to receive credit for their annual physical exams and biometric values on www.mycigna.com. Web wellness screening information customer signature (required). Include the date and place your e. You can also call us at 1.800.754.3207 to file your claim with one of our claim specialists. Please be sure to write clearly, sign and date the form. 00:01:05) infographic | april 2020 real solutions for real life. Submit your support id is: Cigna group account number on id card Involved parties names, addresses and numbers etc. Fill in the empty fields;
Cigna supplemental health solutions, p.o. Forms without a signature and date are incomplete. Web annual physical exam/wellness screening form harris health system employees and spouses now have the option to use this custom wellness screening form to receive credit for their annual physical exams and biometric values on www.mycigna.com. Please submit your claim through new york life. Submit your support id is: Web wellness screening form patient’s first name mi patient’s last name street address, apt number, po box city state zip patient date of birth mm dd yyyy preferred telephone number is this a home social security (ssn) last 4 numbers patient’s cigna id number on id card or cell number? If you have any questions, please call 888.992.4462. Mm dd yyyy today’s date mm dd yyyy today’s date forms may be sent by: Earn at least 500 additional wellness points through programs and activities (750 total wellness points) Open it using the online editor and begin altering.
Wellness Screening Form Care Fill Out and Sign Printable PDF Template
Include the date and place your e. Registrarse en español your online account gives you access to these features: View claims see a list of your most recent claims, their status, and reimbursements. Web accidental injury, critical illness, hospital care, and wellness incentive claim forms. Web annual physical exam/wellness screening form harris health system employees and spouses now have the.
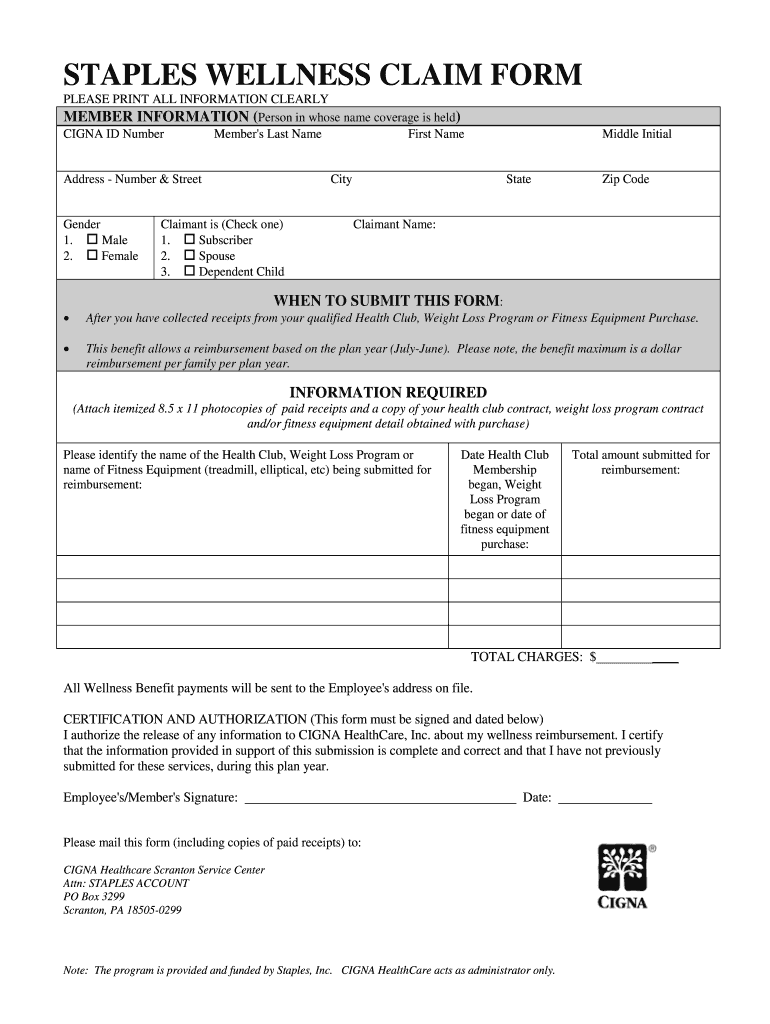
Staples Wellness Claim Form Fill Out and Sign Printable PDF Template
Fill in the empty fields; Please be sure to write clearly, sign and date the form. You are not required to use this form to receive credit for your annual physical. Residence pcp office facility telehealth (audiovisual only) 360 annual wellness examother source patient other (name & relationship) sex at birth: Please submit your claim through new york life.

Cigna Authorization Form Humira Fill Online, Printable, Fillable
Web doing something meaningful starts with a simple decision, a commitment to changing lives. Concerned parties names, places of residence and phone numbers etc. Cigna supplemental health solutions, p.o. Submit your support id is: Please submit your claim through new york life.

Fill Free fillable Cigna
Submit your support id is: Web wellness screening form patient’s first name mi patient’s last name street address, apt number, po box city state zip patient date of birth mm dd yyyy preferred telephone number is this a home social security (ssn) last 4 numbers patient’s cigna id number on id card or cell number? My signature means that the.

Fill Free fillable Cigna Medicare Providers PDF forms
Open it with online editor and begin adjusting. Cigna group account number on id card Customize the blanks with unique fillable areas. Web oral cavity and nasopharyngeal cancers screening (pdq®): Mm dd yyyy today’s date mm dd yyyy today’s date forms may be sent by:
Cigna Colorado Gerontological Society
Complete the mycigna online health assessment (250 wellness points) step 2: Customize the blanks with unique fillable areas. Web wellness screening information customer signature (required). Learn more about careers at the cigna group and apply today. Residence pcp office facility telehealth (audiovisual only) 360 annual wellness examother source patient other (name & relationship) sex at birth:
MotivateMe Wellness Screening Form Cigna Page 2
Web mail your claim form to: Haven’t created an account yet? If you have any questions, please call 888.992.4462. Concerned parties names, places of residence and phone numbers etc. Customize the blanks with unique fillable areas.

Cigna Cigna Healthcare Of California
Web annual physical exam/wellness screening form harris health system employees and spouses now have the option to use this custom wellness screening form to receive credit for their annual physical exams and biometric values on www.mycigna.com. Earn at least 500 additional wellness points through programs and activities (750 total wellness points) Concerned parties names, places of residence and phone numbers.
Cigna Health Organization Logo Editorial Stock Image Image of funding
Fill in the blank areas; Change the template with exclusive fillable fields. Web annual physical exam/wellness screening form harris health system employees and spouses now have the option to use this custom wellness screening form to receive credit for their annual physical exams and biometric values on www.mycigna.com. Forms without a signature and date are incomplete. Registrarse en español your.
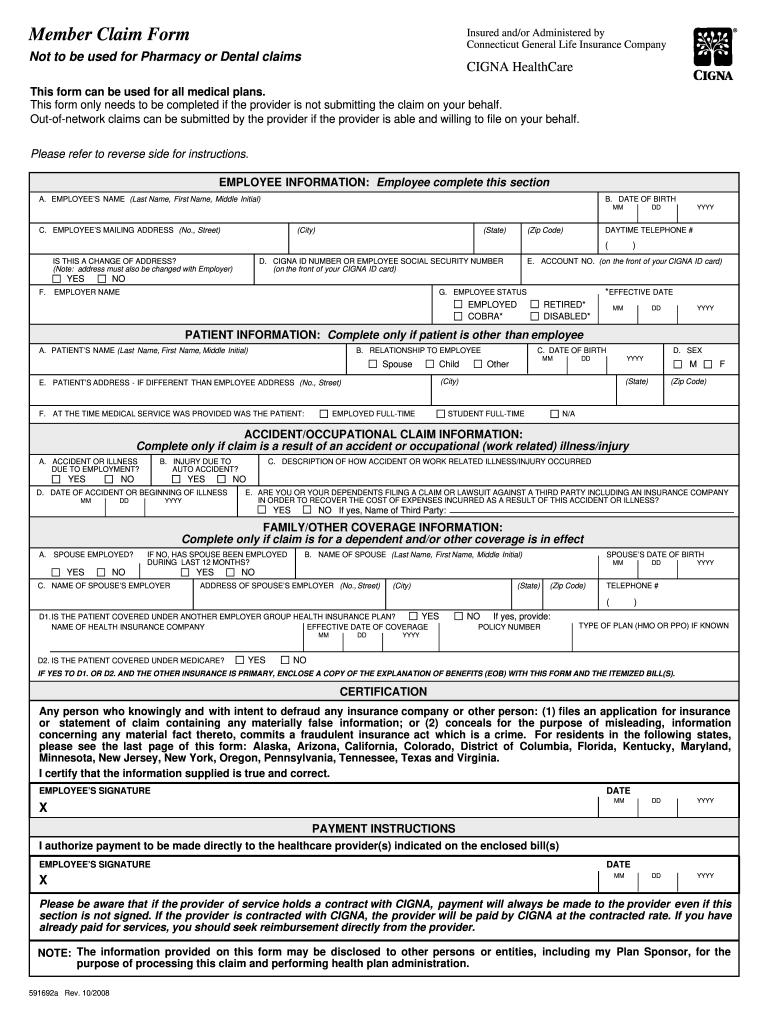
Claim Cigna Fill Out and Sign Printable PDF Template signNow
Open it with online editor and begin adjusting. Web wellness screening form patient’s first name mi patient’s last name street address, apt number, po box city state zip patient date of birth mm dd yyyy preferred telephone number is this a home social security (ssn) last 4 numbers patient’s cigna id number on id card or cell number? Residence pcp.
Accidental Injury Claim Form [Pdf] Critical Illness Claim Form [Pdf] Hospital Care Claim Form [Pdf] Wellness Incentive Claim Form [Pdf] Life, Ad&D, Or Disability Claims.
Web wellness screening information customer signature (required). New york paid family leave forms View claims see a list of your most recent claims, their status, and reimbursements. Learn more about careers at the cigna group and apply today.
Web Find The Cigna Wellness Screening Form You Want.
Cigna supplemental health solutions, p.o. Web annual physical exam/wellness screening form harris health system employees and spouses now have the option to use this custom wellness screening form to receive credit for their annual physical exams and biometric values on www.mycigna.com. Haven’t created an account yet? Web accidental injury, critical illness, hospital care, and wellness incentive claim forms.
Please Submit Your Claim Through New York Life.
Web mail your claim form to: Mm dd yyyy today’s date mm dd yyyy today’s date forms may be sent by: Web how to file a claim for wellness incentive benefits cigna accidental injury insurance your cigna accidental injury insurance plan comes with a wellness incentive benefit. Involved parties names, addresses and numbers etc.
Web Doing Something Meaningful Starts With A Simple Decision, A Commitment To Changing Lives.
My signature means that the information on this form is correct. Earn at least 500 additional wellness points through programs and activities (750 total wellness points) Submit your support id is: 00:01:05) infographic | april 2020 real solutions for real life.