Ambetter Appeal Form
Ambetter Appeal Form - Web outpatient prior authorization fax form (pdf) outpatient treatment request form (pdf) provider fax back form (pdf) applied behavioral analysis authorization form (pdf). Web appeal by phone, fax, or in person. All fields are required information. Web a request for reconsideration. Web to ensure that ambetter member’s rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Web use this form as part of the ambetter from superior healthplanrequest for reconsideration and claim dispute process. Web all ambetter from arizona complete health members are entitled to a complaint/grievance and appeals process if a member is displeased with any aspect of services rendered. Box 277610 sacramento, ca 95827 fax you may also fax. Web grievance or appeal form. Use your zip code to find your personal plan.
If you choose not to complete this form, you may write a letter that includes. See coverage in your area; The procedures for filing a. Web 2023 provider and billing manual (pdf) 2022 provider and billing manual (pdf) provider manual addendum (pdf) prior authorization guide (pdf) payspan (pdf) quick. Web appeal by phone, fax, or in person. Disputes of denials for code editing policy. Use your zip code to find your personal plan. Web you will find forms that you can use for your appeal in the member information packet, you will find forms you can use for your appeal. All fields are required information. The completed form or your letter should be mailed to:.
Web outpatient prior authorization fax form (pdf) outpatient treatment request form (pdf) provider fax back form (pdf) applied behavioral analysis authorization form (pdf). Box 277610 sacramento, ca 95827 fax you may also fax. Web appeal by phone, fax, or in person. The procedures for filing a. Web you will find forms that you can use for your appeal in the member information packet, you will find forms you can use for your appeal. If you choose not to complete this form, you may write a letter that includes. Web to ensure that ambetter member's rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Web grievance or appeal form. If you wish to file a grievance or an appeal, please complete this form. The procedures for filing a.
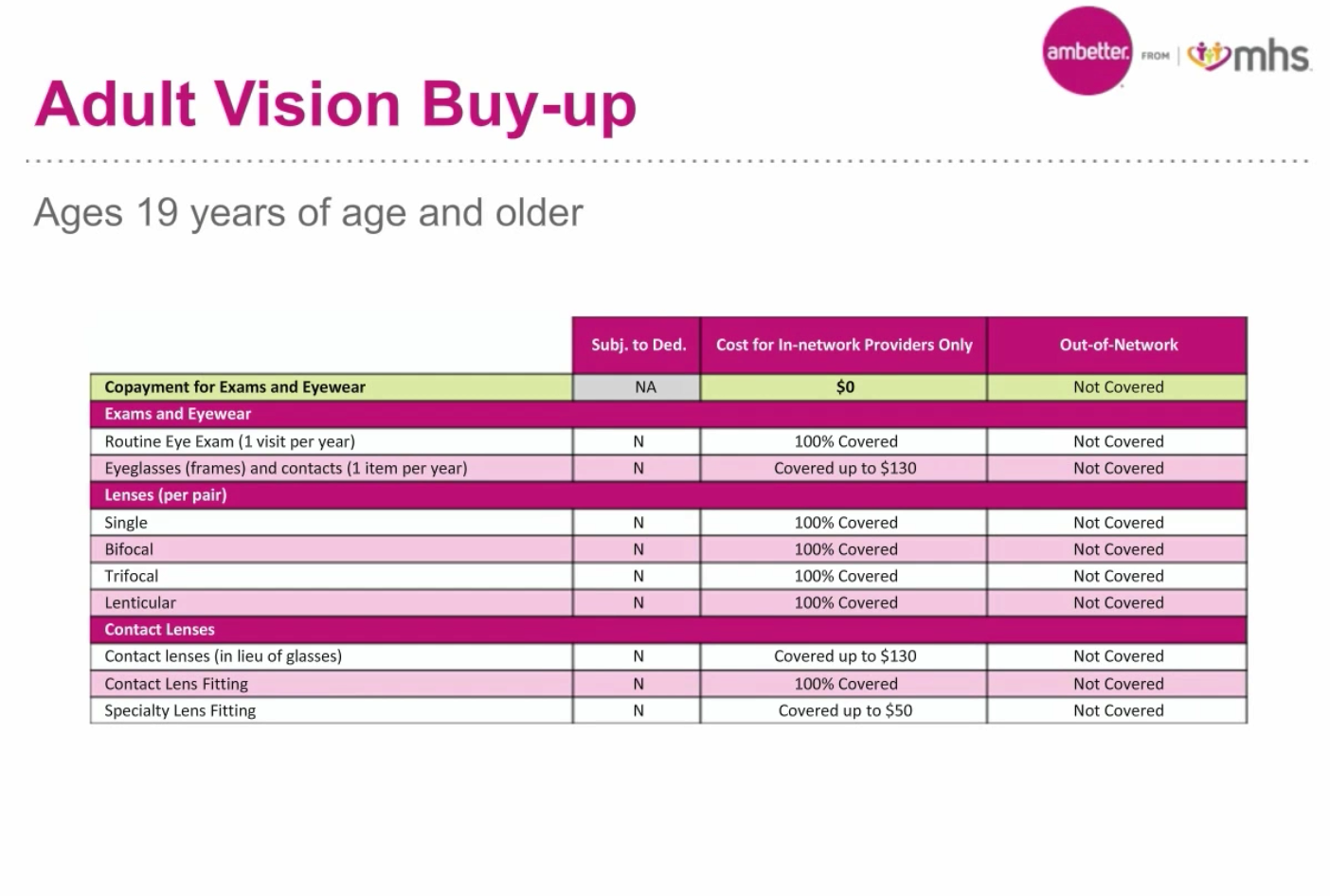
What are Ambetter Indiana's Dental and Vision Benefits? Independent
The procedures for filing a. The completed form can be returned by mail or fax. Web grievance or appeal form. Web appeal by phone, fax, or in person. If you choose not to complete this form, you may write a letter that includes the information requested below.

Who Accepts Ambetter Health Insurance insurance
If you choose not to complete this form, you may write a letter that includes the information requested below. Use your zip code to find your personal plan. Azch developed these forms to help. Ambetter from health net attn: Web you can mail a written appeal or grievance to:

Buckeye Health Plan Waiver Provider Instructions & Application Fill
The procedures for filing a. Web a request for reconsideration. If you choose not to complete this form, you may write a letter that includes the information requested below. If you do not have access to a phone, you can complete this form or write a letter. Web grievance or appeal form.

What Is The Group Id For Ambetter Health Net Commercial Ca If you
Web grievance or appeal form. The completed form can be returned by mail or fax. Web to ensure that ambetter member’s rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Web a request for reconsideration. All fields are required information.

Online form to cancel your ambetter contract
Web outpatient prior authorization fax form (pdf) outpatient treatment request form (pdf) provider fax back form (pdf) applied behavioral analysis authorization form (pdf). Web appeal by phone, fax, or in person. If you choose not to complete this form, you may write a letter that includes the information requested below. Ambetter from health net attn: If you choose not to.

Envolve Vision Newsletter Volume 6 Issue 3 National English
All fields are required information. Web to ensure that ambetter member's rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Use your zip code to find your personal plan. 1) a copy of the eop(s) with the claim numbers to be adjudicated clearly circled 2) the response to your original request. If you choose not.
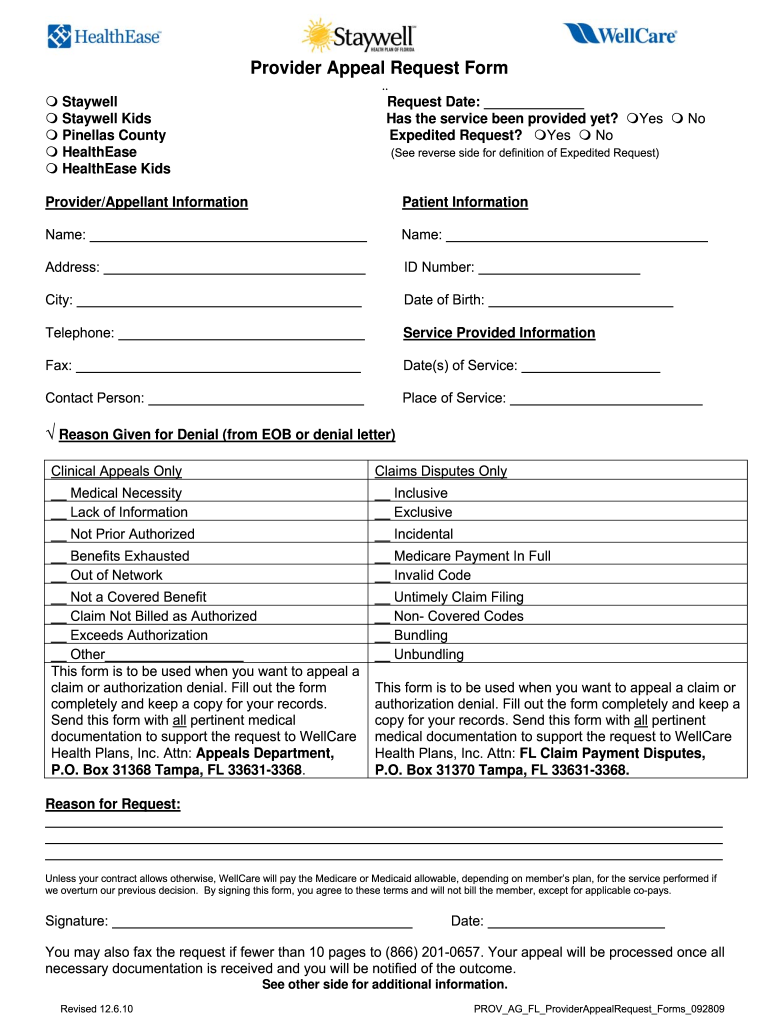
Wellcare Appeal Form Fill Online, Printable, Fillable, Blank pdfFiller
If you wish to file a grievance or an appeal, please complete this form. Appeals & grievances department p.o. Web grievance or appeal form. Web you will find forms that you can use for your appeal in the member information packet, you will find forms you can use for your appeal. Web a request for reconsideration.

Gallery of Ambetter Prior Authorization form Beautiful Kircblog 2015
If you do not have access to a phone, you can complete this form or write a letter. All fields are required information. Web you can mail a written appeal or grievance to: Use your zip code to find your personal plan. Web to ensure that ambetter member’s rights are protected, all ambetter members are entitled to a complaint/grievance and.

Ambetter Health Insurance Coverage For Drug Rehab
Web you can mail a written appeal or grievance to: Web you will find forms that you can use for your appeal in the member information packet, you will find forms you can use for your appeal. Web grievance or appeal form. If you do not have access to a phone, you can complete this form or write a letter..

Gallery of Ambetter Prior Authorization form Beautiful Kircblog 2015
The procedures for filing a. If you choose not to complete this form, you may write a letter that includes. You must file an appeal within 180 days of the date on the denial letter. Web outpatient prior authorization fax form (pdf) outpatient treatment request form (pdf) provider fax back form (pdf) applied behavioral analysis authorization form (pdf). The completed.
Web Outpatient Prior Authorization Fax Form (Pdf) Outpatient Treatment Request Form (Pdf) Provider Fax Back Form (Pdf) Applied Behavioral Analysis Authorization Form (Pdf).
Web you can mail a written appeal or grievance to: Web grievance or appeal form. All fields are required information. If you do not have access to a phone, you can complete this form or write a letter.
Web Use This Form As Part Of The Ambetter From Superior Healthplanrequest For Reconsideration And Claim Dispute Process.
Web appeal by phone, fax, or in person. You must file an appeal within 180 days of the date on the denial letter. Web you will find forms that you can use for your appeal in the member information packet, you will find forms you can use for your appeal. If you choose not to complete this form, you may write a letter that includes.
Web All Ambetter From Arizona Complete Health Members Are Entitled To A Complaint/Grievance And Appeals Process If A Member Is Displeased With Any Aspect Of Services Rendered.
Web a request for reconsideration. Web to ensure that ambetter member's rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Appeals & grievances department p.o. The procedures for filing a.
Box 277610 Sacramento, Ca 95827 Fax You May Also Fax.
1) a copy of the eop(s) with the claim numbers to be adjudicated clearly circled 2) the response to your original request. If you choose not to complete this form, you may write a letter that includes the information requested below. Disputes of denials for code editing policy. Use your zip code to find your personal plan.