Aetna Medicare Appeal Form For Providers
Aetna Medicare Appeal Form For Providers - You must complete this form. To obtain a review, you’ll need to submit this form. Web complaint and appeal form. Aetna medicare part c appeals & grievances po box 14067 lexington, ky 40512. As an aetna dentist, you'll be part of a strong national network with access to millions of members. Because the society ditches office work, the completion of paperwork more and. Web complaint and appeal request note: These changes do not affect member appeals. Make sure to include any information. Or use our national fax number:
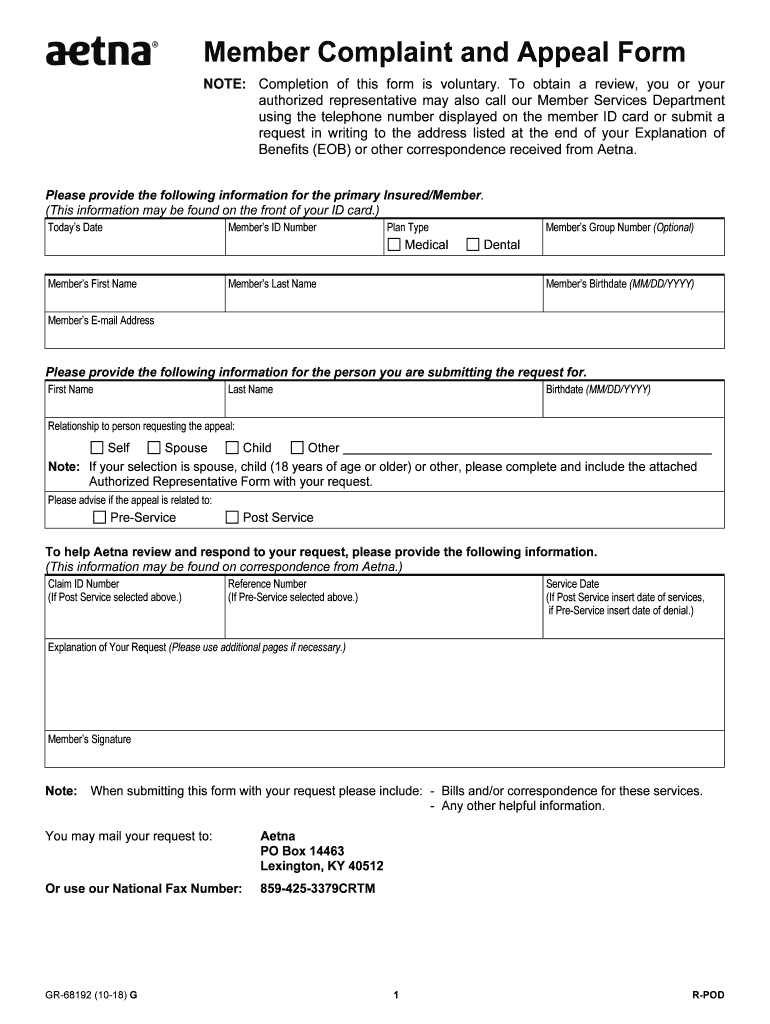
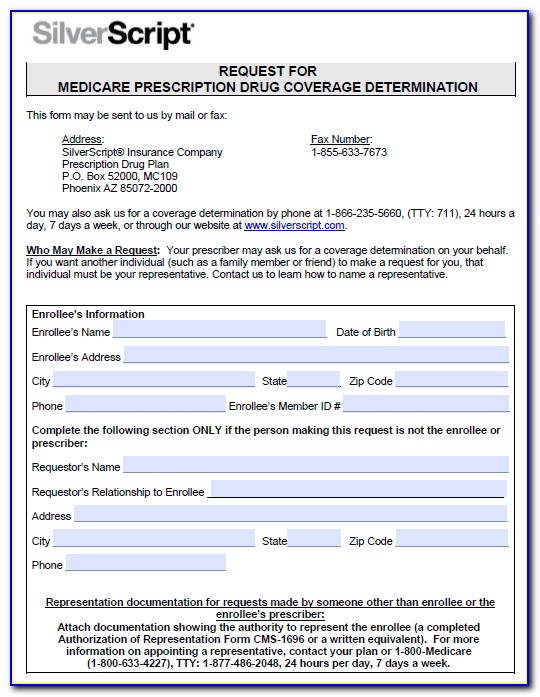
In some cases, we may allow exceptions for a. Ask for coverage of a medical service or prescription drug. Exceptions apply to members covered under. Web providers in the aetna network have the right to appeal denied medical item or service authorizations or medicare part b prescription drug for members. Because aetna medicare (or one of our delegates) denied your request for payment of. Web plan type member’s group number (optional) medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) to help us review and. Who may make a request: Web 4.8 satisfied 375 votes what makes the aetna provider complaint and appeal form legally binding? Your doctor may ask us for an appeal on your behalf. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form.
Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. These changes do not affect member appeals. Web provider appeals dispute & appeal process: Aetna medicare part c appeals & grievances po box 14067 lexington, ky 40512. Web reconsiderations can be submitted online, by phone or by mail/fax. You may mail your request to: Web as an aetna medicare member, you have the right to: Exceptions apply to members covered under. Ask for coverage of a medical service or prescription drug. Web you can call us at:
Aetna better health prior authorization form Fill out & sign online
Aetna medicare part c appeals & grievances po box 14067 lexington, ky 40512. You must complete this form. Web your denial to ask us for an appeal. As an aetna dentist, you'll be part of a strong national network with access to millions of members. Ask for coverage of a medical service or prescription drug.
Aetna GR69250 2019 Fill and Sign Printable Template Online US
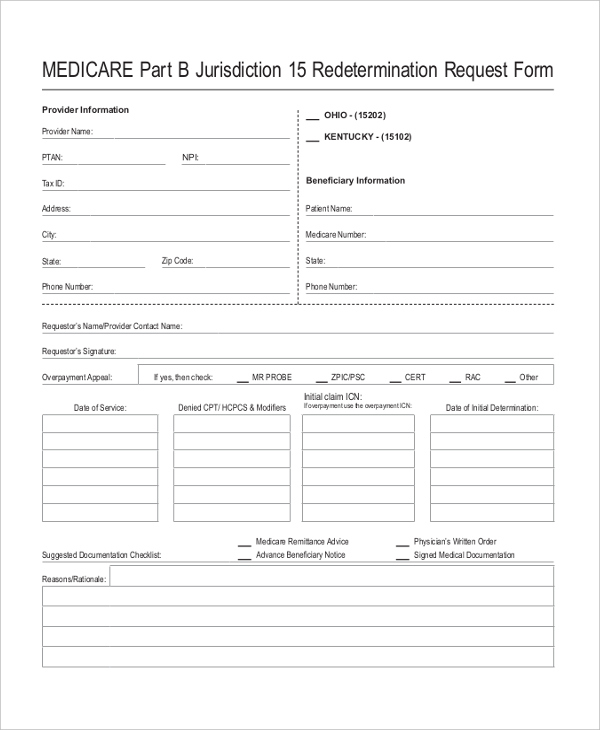
Web request for an appeal of an aetna medicare advantage (part c) plan claim denial. Web provider appeals dispute & appeal process: Web as an aetna medicare member, you have the right to: In some cases, we may allow exceptions for a. Aetna is the brand name used for products and services provided by one or more of the aetna.
Medicare Medical Claim Reimbursement Form Aetna Form Resume
Who may make a request: To obtain a review, you’ll need to submit this form. Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its. Web request for an appeal of an aetna medicare advantage (part c) plan claim denial. Make sure.

Prior Authorization Form For Medicare Advantage Universal Network
You must complete this form. Make sure to include any information. Appeals must be submitted by mail/fax, using the provider complaint and appeal form. Web you can call us at: Web providers in the aetna network have the right to appeal denied medical item or service authorizations or medicare part b prescription drug for members.
Aetna Medicare Complaint Team Fill Out and Sign Printable PDF
Web request for an appeal of an aetna medicare advantage (part c) plan claim denial. Web consumers may call or write the bureau to have claims reviewed. Appeals must be submitted by mail/fax, using the provider complaint and appeal form. These changes do not affect member appeals. Callers outside california and those in california (area codes 213 or 310), may.
Aetna Life Insurance Medicare Supplement Aetna LeClair Group
Web providers in the aetna network have the right to appeal denied medical item or service authorizations or medicare part b prescription drug for members. Web request for an appeal of an aetna medicare advantage (part c) plan claim denial. Aetna is the brand name used for products and services provided by one or more of the aetna group of.
Member aetna com membersecure assets pdfs forms 68192 pdf Fill out
Aetna medicare part c appeals & grievances po box 14067 lexington, ky 40512. Or use our national fax number: In some cases, we may allow exceptions for a. Web provider appeals dispute & appeal process: Web complaint and appeal form.
FREE 10+ Sample Medicare Forms in PDF MS Word
Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its. Web your denial to ask us for an appeal. Aetna medicare part c appeals & grievances po box 14067 lexington, ky 40512. Web 2024 aetna life ins. You may mail your request.

Fill Free fillable Aetna Health Insurance PDF forms
Web consumers may call or write the bureau to have claims reviewed. Web as an aetna medicare member, you have the right to: Or use our national fax number: In some cases, we may allow exceptions for a. Web your denial to ask us for an appeal.
Aetna Medicare Medication Prior Authorization Form Form Resume
In some cases, we may allow exceptions for a. (this information may be found on the front of the member’s id card.) today’s date member’s id number plan type member’s group. Exceptions apply to members covered under. Callers outside california and those in california (area codes 213 or 310), may contact the consumer. Web plan type member’s group number (optional).
You May Mail Your Request To:
Web please provide the following information. Web plan type member’s group number (optional) medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) to help us review and. Web you can call us at: Web your denial to ask us for an appeal.
To Obtain A Review, You’ll Need To Submit This Form.
Payment appeals for contracted provider requests. Who may make a request: Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. As an aetna dentist, you'll be part of a strong national network with access to millions of members.
Web Request For An Appeal Of An Aetna Medicare Advantage (Part C) Plan Authorization Denial.
Web as an aetna medicare member, you have the right to: Web 2024 aetna life ins. If you have a dispute around the rate used for payment. % change approved status effective date aetna life.
Web 4.8 Satisfied 375 Votes What Makes The Aetna Provider Complaint And Appeal Form Legally Binding?
Web complaint and appeal request note: Because aetna medicare (or one of our delegates) denied your request for. Web complaint and appeal form. This form may be sent to us by mail or fax: