Aetna Aor Form
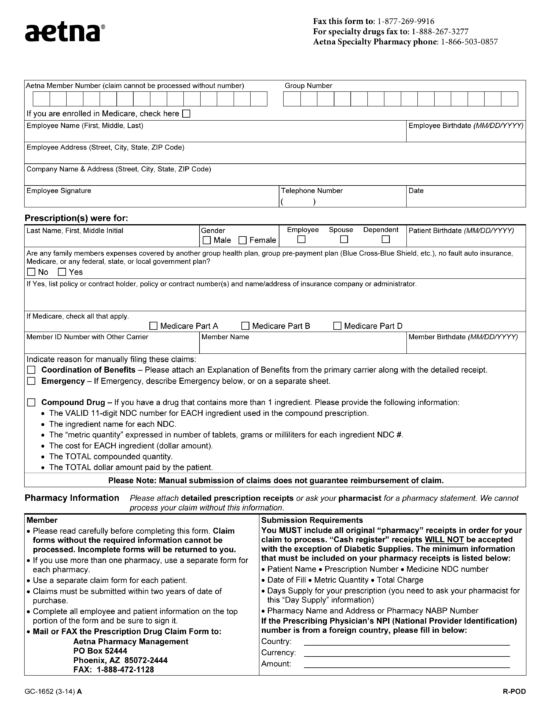
Aetna Aor Form - Web fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness reimbursement you paid a doctor,. We recently updated our aor reassignment policy in the aetna medicare producer guide. Prescription drug mail order form. Sign it in a few clicks draw your. Web appointment of representative form. Hospice part d exception form. Web by signing this form i authorize aetna to disclose information below for the following purpose. Fill in your first name, last name, address information, date of birth and your. Medicare drug coverage determination form. To be completed by the party seeking representation (i.e., the medicare beneficiary, the provider or the supplier):
Waiver of liability (wol) form. Below are a list of important member forms: Fill in your first name, last name, address information, date of birth and your. Medicare drug coverage determination form. How to fill out the appointment of representative form aetna. Check one of the following options: We recently updated our aor reassignment policy in the aetna medicare producer guide. To be completed by the party seeking representation (i.e., the medicare beneficiary, the provider or the supplier): Prior authorization form (see attached prior. Web fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness reimbursement you paid a doctor,.
Check one of the following options: Web fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness reimbursement you paid a doctor,. Fill in your first name, last name, address information, date of birth and your. Prescription drug mail order form. Web aetna better health® of illinois 333 w. Web find the insurance documents you need, including claims, tax, reimbursement and other health care forms. Fill out to enroll in one of the aetna medicare dual eligible special needs plans (hmo d. Web appointment of representative form. To be completed by the party seeking representation (i.e., the medicare beneficiary, the provider or the supplier): Medicare drug coverage determination form.
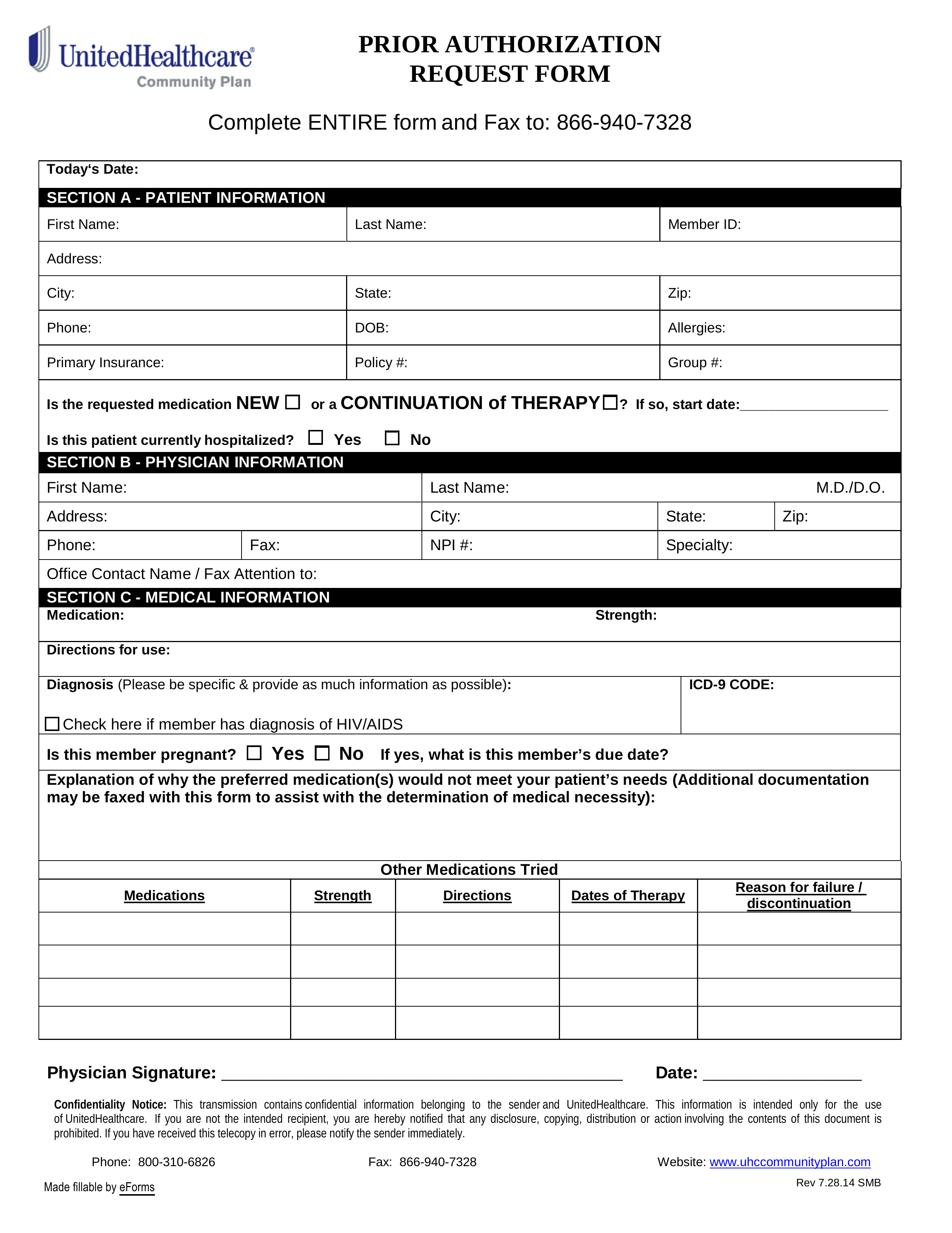
Free UnitedHealthcare Prior (Rx) Authorization Form PDF eForms
Also learn how to find forms customized specifically for your aetna. The completed and signed form is valid for one (1) year. We recently updated our aor reassignment policy in the aetna medicare producer guide. Medicare drug coverage determination form. Web review changes to the agent of record (aor) reassignment policy.
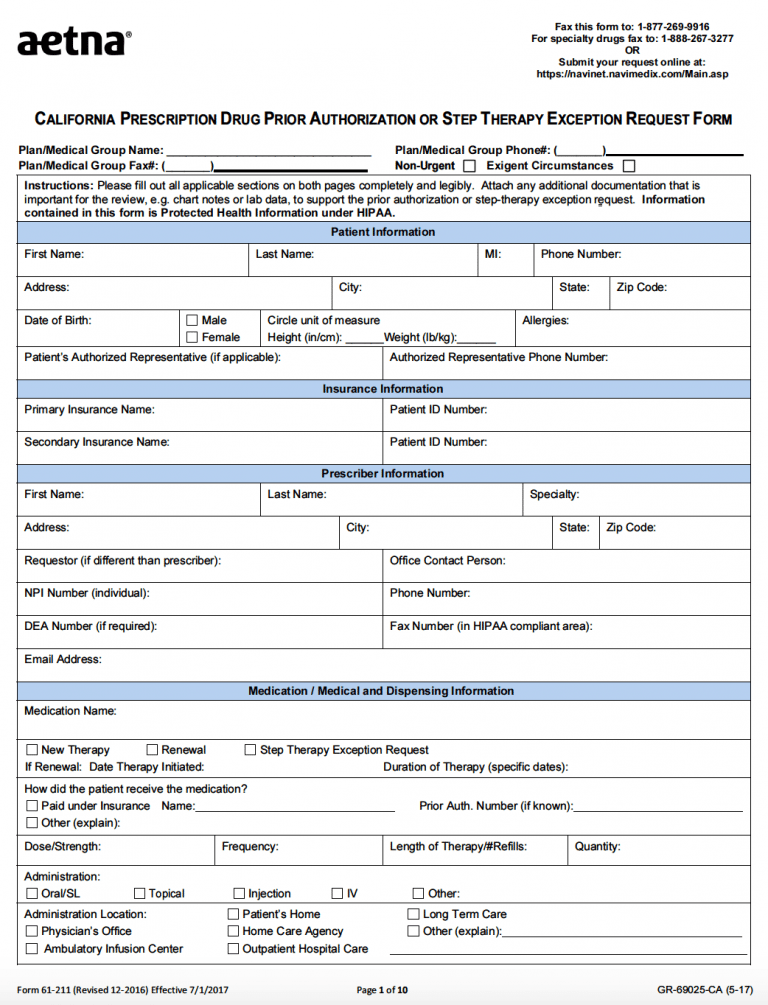
Free AETNA Prior Prescription (Rx) Authorization Form PDF
Edit your aetna medicare aor form online type text, add images, blackout confidential details, add comments, highlights and more. Waiver of liability (wol) form. Web appointment of representative form. Below are a list of important member forms: Fill in your first name, last name, address information, date of birth and your.

What is the full form of AM and PM AM aor PM Ka matlab Kiya hei
Web review changes to the agent of record (aor) reassignment policy. Also learn how to find forms customized specifically for your aetna. Check one of the following options: Hospice part d exception form. Medicare drug coverage determination form.
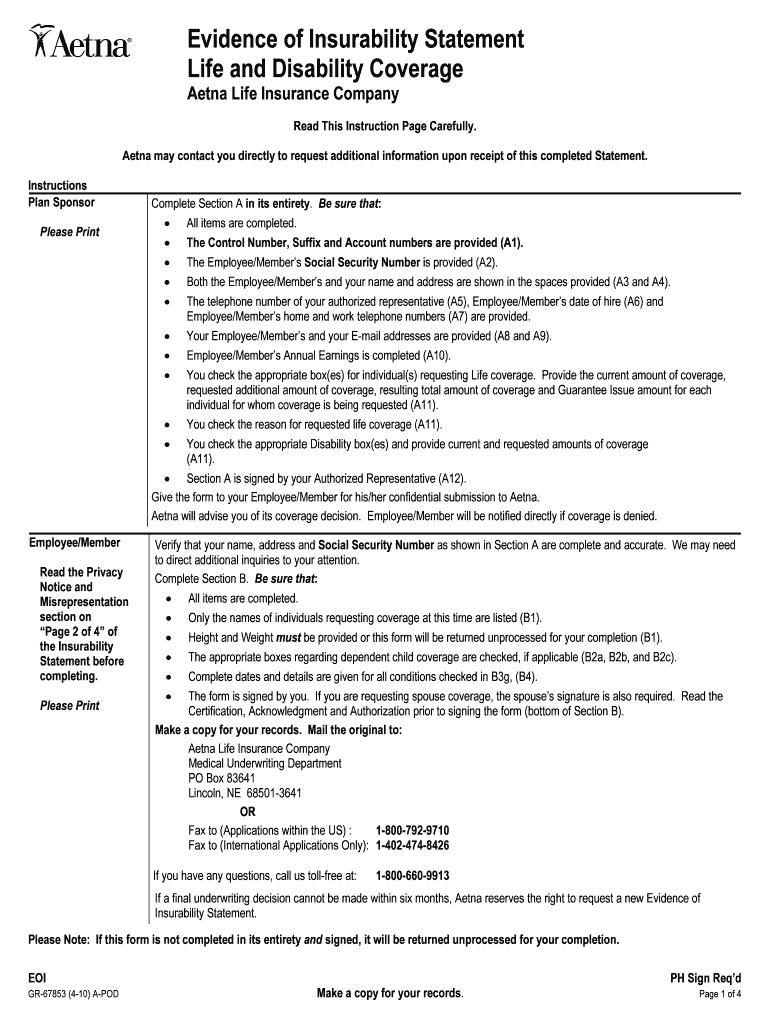
Eoi Form Fill Out and Sign Printable PDF Template signNow
Sign it in a few clicks draw your. Medicare drug coverage determination form. Web health insurance plans | aetna Web find the aetna medicare forms you need to help you get started with claims reimbursements, aetna rx home delivery, filing an appeal and more. To be completed by the party seeking representation (i.e., the medicare beneficiary, the provider or the.

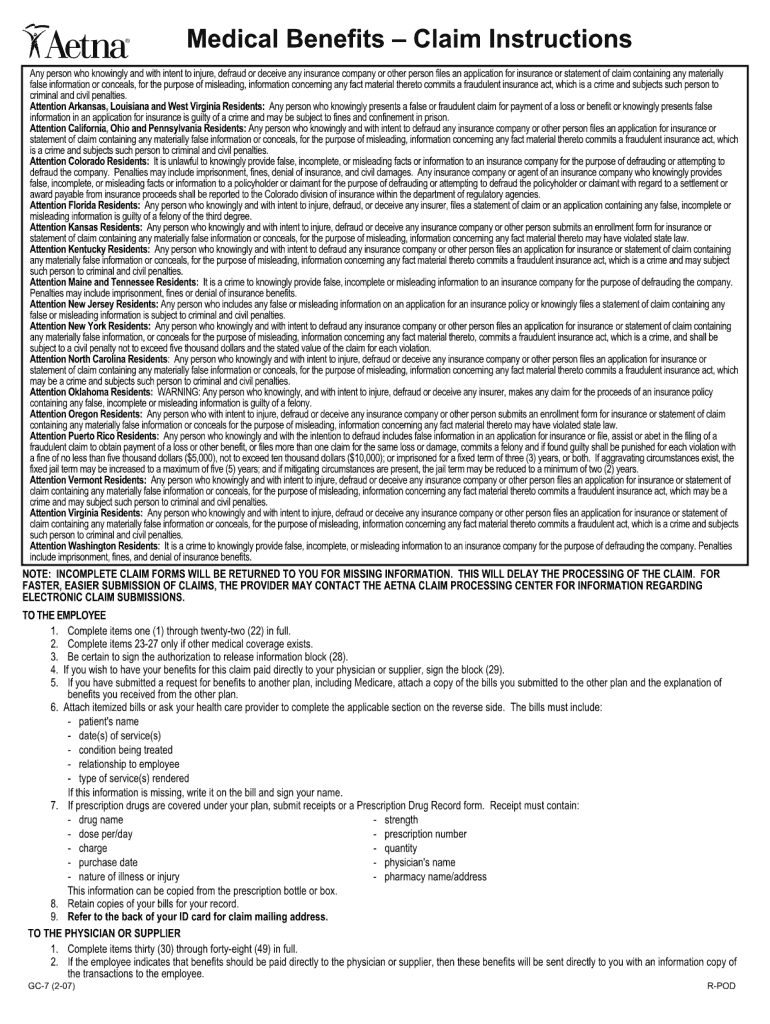
Aetna Facility Form Fill Online, Printable, Fillable, Blank pdfFiller
Aetna's online service center developed to meet the informational needs of our producers, general agents and firm employees including access to: Also learn how to find forms customized specifically for your aetna. Community behavioral health authorization form. We recently updated our aor reassignment policy in the aetna medicare producer guide. Prescription drug mail order form.

Acknowledgement of Risk Form Career & Internship Center University
Web find the aetna medicare forms you need to help you get started with claims reimbursements, aetna rx home delivery, filing an appeal and more. Hospice part d exception form. Community behavioral health authorization form. Sign it in a few clicks draw your. Waiver of liability (wol) form.
Aetna Eylea Prior Authorization Form Fill Out and Sign Printable PDF
To be completed by the party seeking representation (i.e., the medicare beneficiary, the provider or the supplier): Edit your aetna medicare aor form online type text, add images, blackout confidential details, add comments, highlights and more. Web find the insurance documents you need, including claims, tax, reimbursement and other health care forms. Web back to cms forms list; Web review.
Free Aetna Prior (Rx) Authorization Form PDF eForms
Web find the insurance documents you need, including claims, tax, reimbursement and other health care forms. Hospice part d exception form. Web aetna better health® of illinois 333 w. Edit your aetna medicare aor form online type text, add images, blackout confidential details, add comments, highlights and more. Check one of the following options:
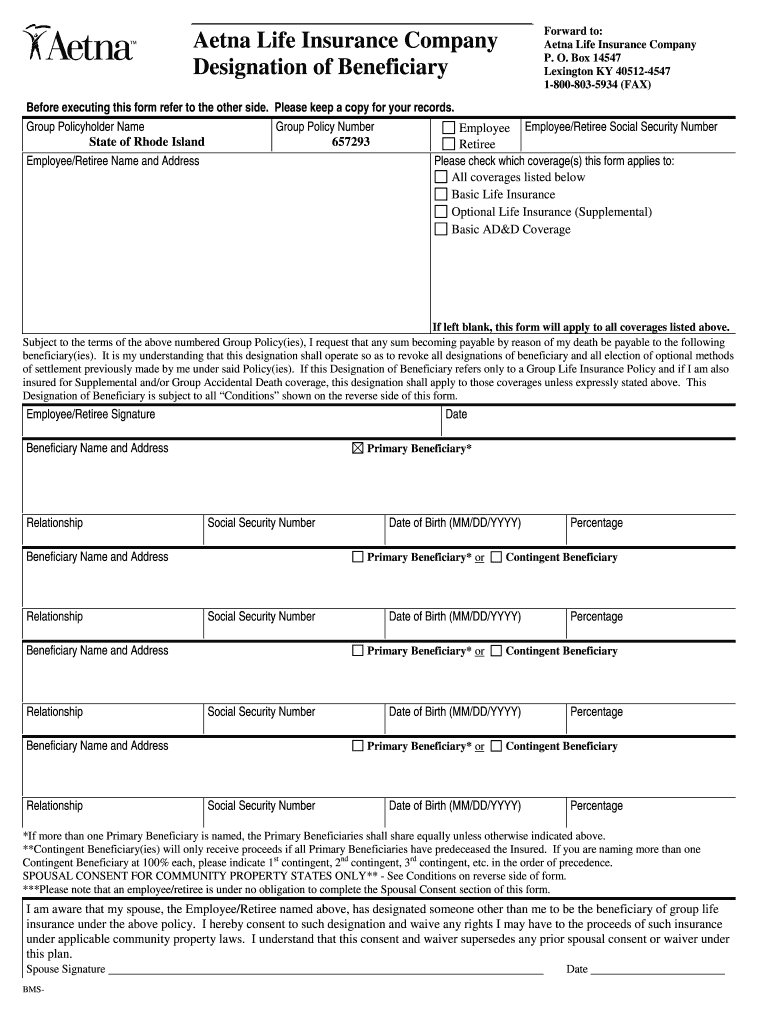
Aetna Designation of Beneficiary Fill and Sign Printable Template
We recently updated our aor reassignment policy in the aetna medicare producer guide. Prescription drug mail order form. Edit your aetna medicare aor form online type text, add images, blackout confidential details, add comments, highlights and more. Waiver of liability (wol) form. Medicare drug coverage determination form.
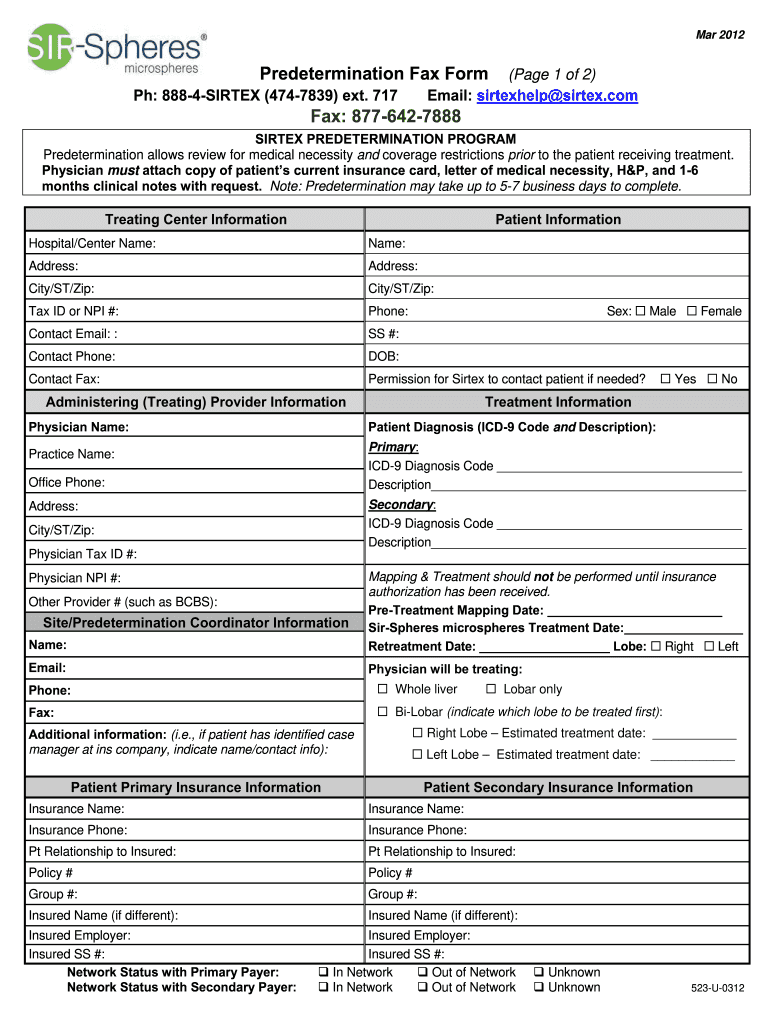
Aetna Predetermination Form Fill Out and Sign Printable PDF Template
Web back to cms forms list; Web appointment of representative form. Prescription drug mail order form. Prior authorization form (see attached prior. Community behavioral health authorization form.
Fill Out To Enroll In One Of The Aetna Medicare Dual Eligible Special Needs Plans (Hmo D.
Prior authorization form (see attached prior. Wacker drive suite 2100 chicago, il 60606 tel: Cms 1696 dynamic list information. The completed and signed form is valid for one (1) year.
Waiver Of Liability (Wol) Form.
Below are a list of important member forms: Community behavioral health authorization form. Web appointment of representative form. We recently updated our aor reassignment policy in the aetna medicare producer guide.
Web The Form Must Be Signed By You And By The Person Whom You Would Like To Act On Your Behalf.
Hospice part d exception form. Prescription drug mail order form. Fill in your first name, last name, address information, date of birth and your. Sign it in a few clicks draw your.
Web Review Changes To The Agent Of Record (Aor) Reassignment Policy.
Check one of the following options: Web back to cms forms list; Web by signing this form i authorize aetna to disclose information below for the following purpose. Web aetna better health® of illinois 333 w.