Ada Claim Form Pdf
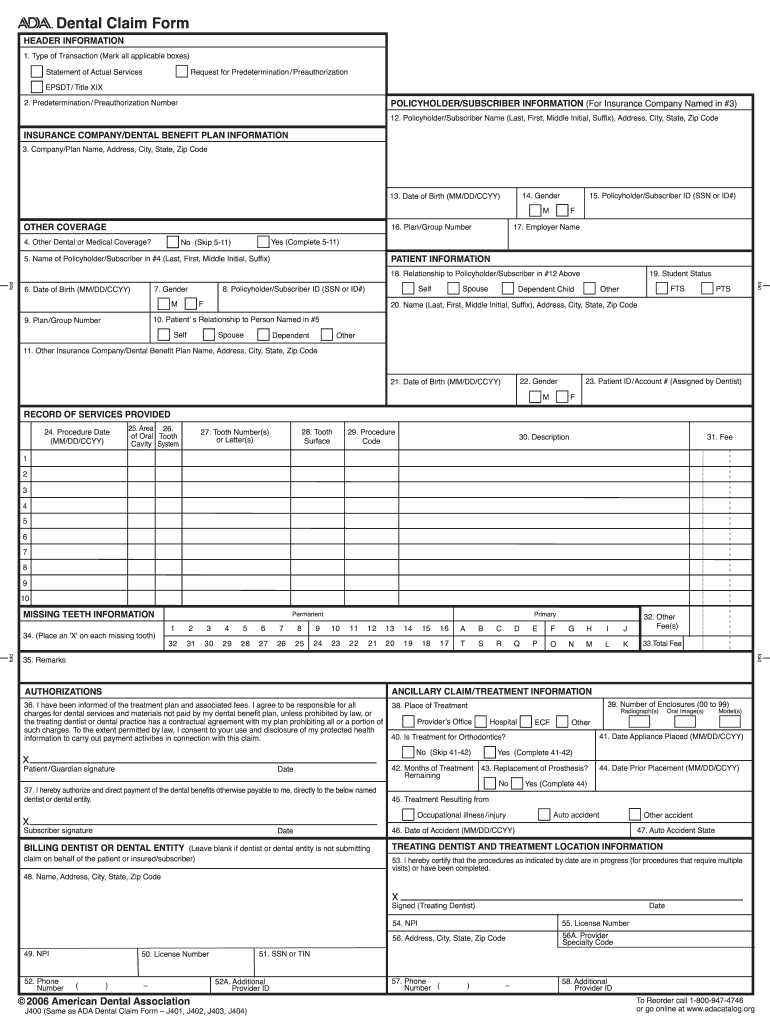
Ada Claim Form Pdf - Version 2024 © american dental association. I have been informed of the treatment plan and associaled fees. Web authorizations ancillary claim/treatment information 36. Department of justice civil rights division 950 pennsylvania avenue, nw washington, dc 20530 3. Web view ada_claimform.pdf from maa 103 at carrington college, sacramento. Gender m f m f u Such fees include state taxes, where applicable, and other fees imposed by regulatory bodies. Numberof enclosures (00 to 99) charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or o Comprehensive ada dental claim form completion instructions are printed in the cdt manual. Dental claim form header information 1.
Web comprehensive ada dental claim form completion instructions are printed in the cdt manual. Web dental claim form record of services provided 24. Five relevant extracts from that section follow: Note that data items are in. Numberof enclosures (00 to 99) charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or o Web authorizations ancillary claim/treatment information 36. Easily fill out pdf blank, edit, and sign them. For providers already in calvcb’s system: Type of transaction (mark all applicable boxes) dental claim form statement of actual services epsdt / title 2. Number 48 and number 51 on your bill must match exactly to what is.
Number 48 and number 51 on your bill must match exactly to what is. Total of all fees listed on the claim form. Web authorizations ancillary claim/treatment information 36. Tooth number(s) or letter(s) 28. Report missing teeth on each claim submission. Type of transaction (mark all applicable boxes) request for predetermination / Fee 1 2 3 4 5 6 7 8 9 10 33. Missing teeth information (place an “x” on each missing tooth.) 34. The ada dental claim form is a form that is used to document dental treatment and procedures. Numberof enclosures (00 to 99) charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or o

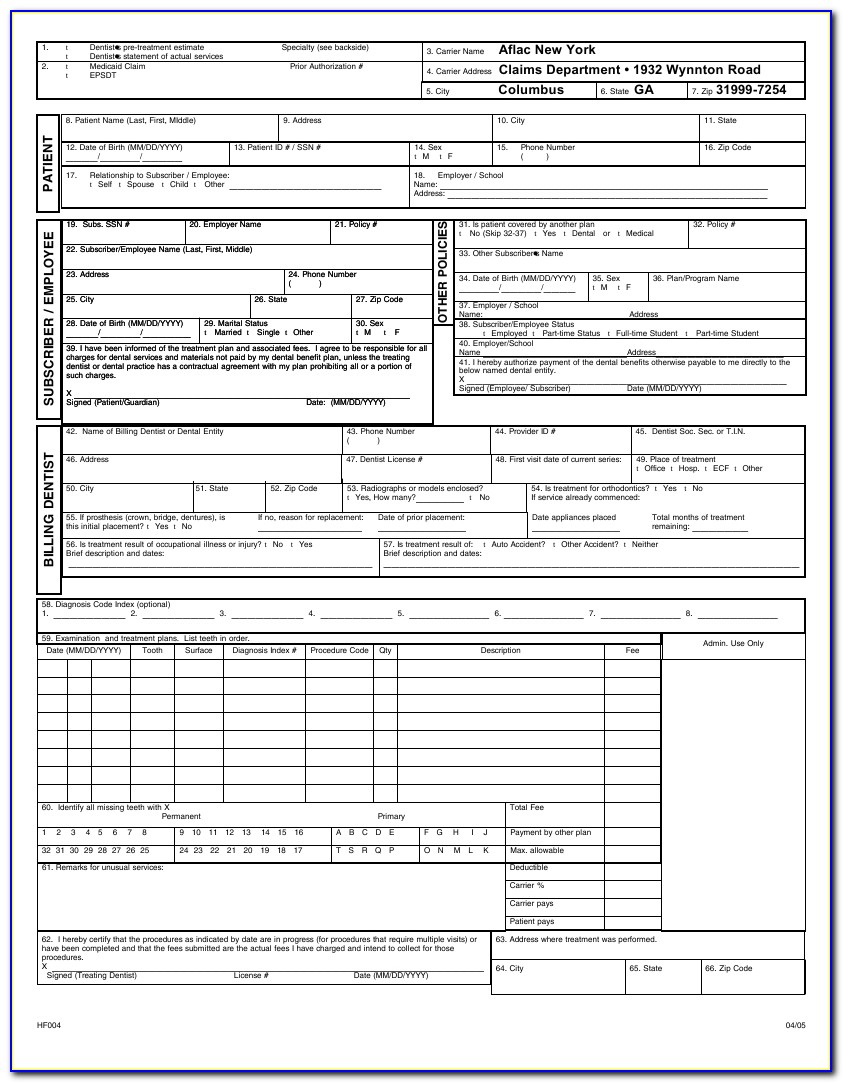
Aetna Medical Claim Form Download the free Printable Basic Blank
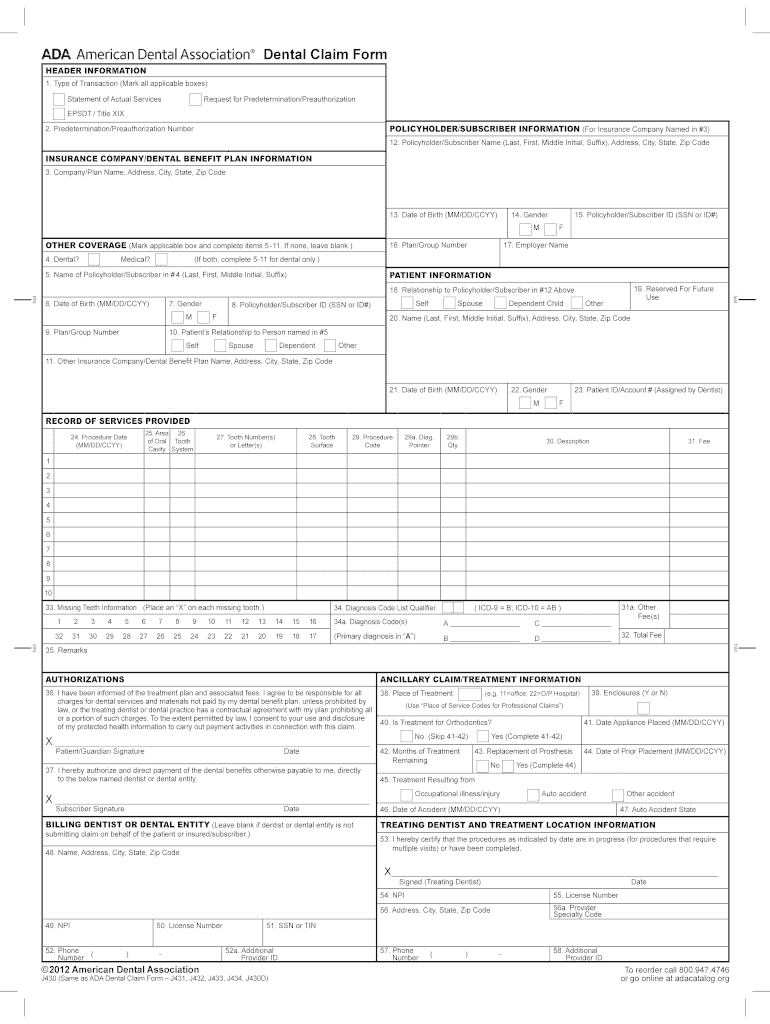
Web ada 2019 claim form for licensees the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into the now current version of the hipaa standard (837d v5010) electronic dental claim. Save or instantly send your ready documents. Five relevant extracts from that section.

Where does box 56a on the ADA claim form come from? Dentrix Ascend
Missing teeth information (place an “x” on each missing tooth.) 34. Gender m f m f u Web are you thinking about getting blank ada dental claim form to fill? Number 48 and number 51 on your bill must match exactly to what is. Web the ada dental claim form provides a common format for reporting dental services to a.
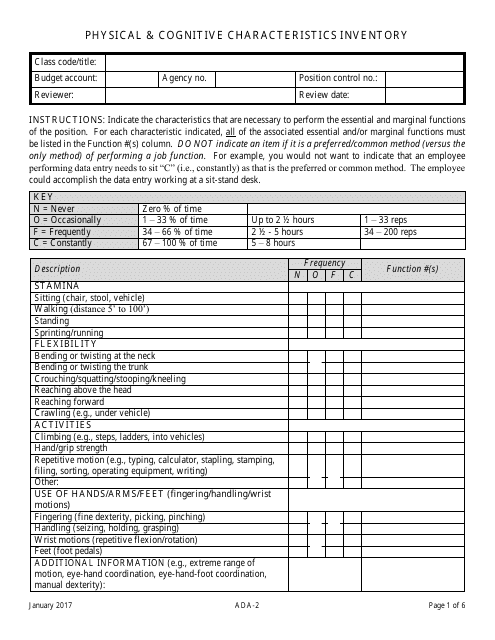
Form ADA2 Download Fillable PDF or Fill Online Physical & Cognitive
Department of justice civil rights division 950 pennsylvania avenue, nw washington, dc 20530 3. Any updates to these instructions will be posted on the ada’s web site (ada.org). Mail fill out and send the paper ada complaint form or a letter containing the same information, to: Area of oral cavity 26. Five relevant extracts from that section follow:
Dental Hipaa Forms Form Resume Examples GwkQM40kWV
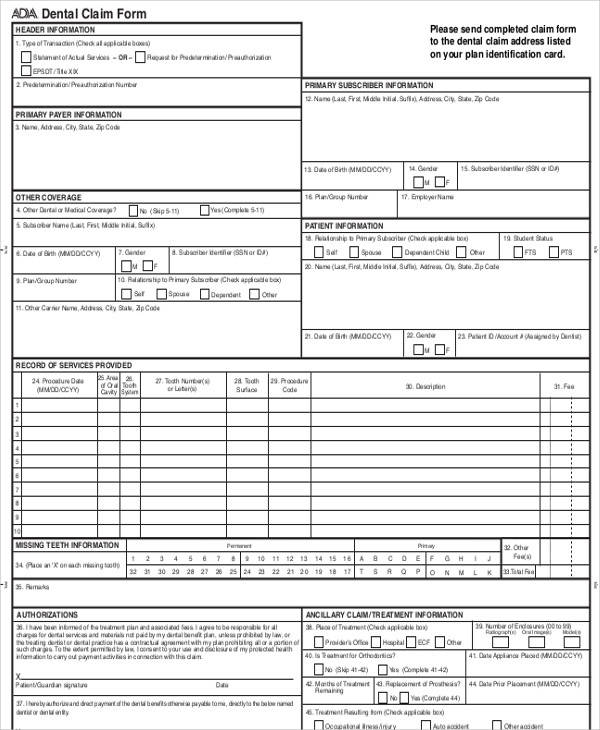
Five relevant extracts from that section follow: Web the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. The ada dental claim form is a form that is used to document dental treatment and procedures. Web authorizations ancillary claim/treatment information 36. Online file a complaint by submitting a report on the.
Dental Claim Forms Pdf Fill Out and Sign Printable PDF Template signNow
The calvcb claim number must be written on the ada dental claim form. Area of oral cavity 26. Version 2024 © american dental association. Save or instantly send your ready documents. Web dental claim form record of services provided 24.
Printable Ada Claim Form 2021 Printable World Holiday
Easily fill out pdf blank, edit, and sign them. Note that data items are in. For providers already in calvcb’s system: Total of all fees listed on the claim form. Missing teeth information (place an “x” on each missing tooth.) 34.
Office Support
Mail fill out and send the paper ada complaint form or a letter containing the same information, to: I have been informed of the treatment plan and associaled fees. Web are you thinking about getting blank ada dental claim form to fill? Web view ada_claimform.pdf from maa 103 at carrington college, sacramento. Total of all fees listed on the claim.

ADA Dental Claim Form Changes Dental Medical Billing
Missing teeth information (place an “x” on each missing tooth.) 34. Easily fill out pdf blank, edit, and sign them. Any updates to these instructions will be posted on the ada’s web site (ada.org). I have been informed of the treatment plan and associaled fees. From voting to parking, the ada is a law that protects people with disabilities in.
Printable Ada Claim Form 2021 Printable World Holiday
I agree to be responsible for all 38. Report missing teeth on each claim submission. I have been informed of the treatment plan and associaled fees. Dental claim form header information 1. Mail fill out and send the paper ada complaint form or a letter containing the same information, to:
ADA Dental Claim Form 2008 Fill and Sign Printable Template Online
Cocodoc is the best website for you to go, offering you a great and easy to edit version of blank ada dental claim form as you desire. Easily fill out pdf blank, edit, and sign them. Five relevant extracts from that section follow: Tooth number(s) or letter(s) 28. Online file a complaint by submitting a report on the department of.
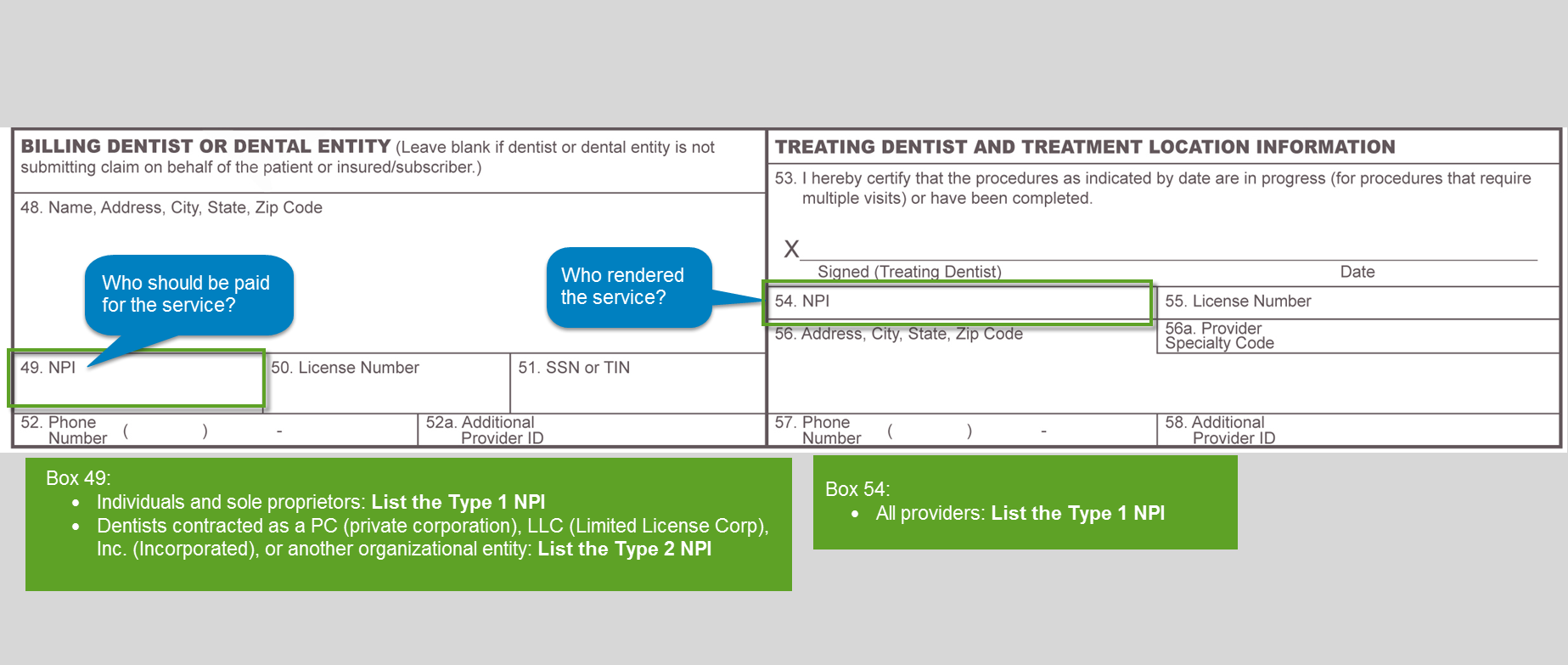
Web Ada Dental Claim Form Sample Unless The Following Sections Of A Dental Bill Are Completed Correctly, The Bill Will Be Returned And Payment May Be Delayed.
Any updates to these instructions will be posted on the ada’s web site (ada.org). Web dental claim form record of services provided 24. Type of transaction (mark all applicable boxes) dental claim form statement of actual services epsdt / title 2. I have been informed of the treatment plan and associaled fees.
The Ada Dental Claim Form Is A Form That Is Used To Document Dental Treatment And Procedures.
Report missing teeth on each claim submission. Web are you thinking about getting blank ada dental claim form to fill? Web object moved this document may be found here Disability rights are civil rights.
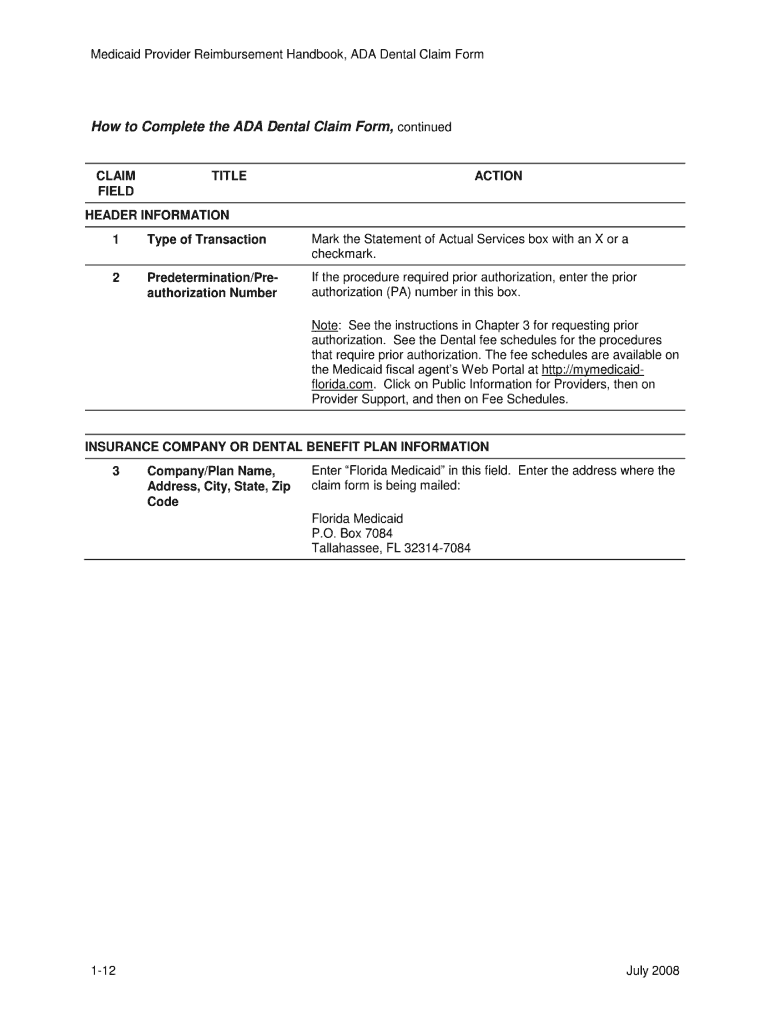
Form Completion Instructions Are Provided For Each Data Item, Which Is Indicated By A Number.
Web ada dental claim form completion instructions. Number 48 and number 51 on your bill must match exactly to what is. Web authorizations ancillary claim/treatment information 36. Fee 1 2 3 4 5 6 7 8 9 10 33.
Ada Policy Promotes Use And Acceptance Of The Most Current Version Of The Ada Dental Claim Form By Dentists And Payers.
Missing teeth information (place an “x” on each missing tooth.) 34. U = unknown coordination of benefits (cob) when a claim is being submitted to the secondary payer, complete the entire form and attach the primary payer’s explanation of benefits (eob) showing the amount paid by the primary payer. Mail fill out and send the paper ada complaint form or a letter containing the same information, to: Numberof enclosures (00 to 99) charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or o